Provider Form
Found 7 free book(s)
Medical Assistance Provider Order Form (Forms Available to ...
www.dhs.pa.govAlso list your Provider Type in the box provided. The forms listed on the left are currently available for ordering. You may order a 3 to 6 month supply of each form. Listed beside each form name is the unit quantity available for ordering. To place an order, please fill in the form number and the quantity desired either in PACKS

IN-HOME SUPPORTIVE SERVICES (IHSS) PROGRAM …
file.lacounty.govIN-HOME SUPPORTIVE SERVICES (IHSS) PROGRAM PROVIDER ENROLLMENT FORM INSTRUCTIONS: † Use black or blue ink to fill out. Print information clearly. † Fill out, sign and return this form in person to the office or location designated by the county. Bring original federal or state government-issued identification and your original Social Security card when returning …

PROVIDER APPLICANT REFERENCE FORM - Florida
apd.myflorida.comJun 01, 2013 · Form 06/01/13 Page 1 of 1 . PROVIDER APPLICANT REFERENCE FORM The applicant below has applied to become a Medicaid Waiver Provider. Your cooperation in completing this reference will greatly assist the Agency for Persons with Disabilities (APD) in determining if the applicant meets the minimum qualifications to become a Waiver Provider ...
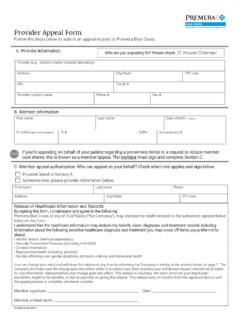
Provider Appeal Form - Premera Blue Cross
www.premera.comProvider listed in Section A Someone else, please provide information below: First name: Last name: Phone: City/State: ZIP code: Release of Healthcare Information and Records . By signing this form, I understand and agree to the following:

Provider Timely Filing Form - triwest.com
www.triwest.comProvider Timely Filing Form. Department of Veterans Affairs (VA) Community Care Network. If you are submitting a claim after the 180-day timely filing deadline because the claim was submitted to the incorrect contractor, please complete this form and include it with the claim submission. The completion of the form is an

Provider Appeal Form - Florida Blue
www-prodstage.bcbsfl.comMail the form and supporting documentation to: Blue Cross and Blue Shield of Florida . Provider Disputes Department . P.O. Box 43237 . Jacksonville, FL 32203-3237 . This address is intended for Provider UM Claim Appeals only. Any other requests will be directed to the appropriate location, which may result in a delay in processing your request.

PROVIDER INQUIRY FORM - Delta Dental
www1.deltadentalins.comProvider disputes will only be processed as a dispute if the provider has first attempted to resubmit the claim for correction or additional review prior to the dispute being filed. Provider disputes receive a written response within 45 days. INQUIRY TYPE: (check one) Claim Resubmission - completed in 30 days or less