
Ambetter Quick Reference Guide
Claim Disputes - (Form located on website) Ambetter from Peach State PO Box 5000 Farmington, MO 63640-5000 . Corrected Claims, Requests for Reconsideration or Claim Disputes: 180 days from the date of explanation of payment or denial is issued . EFT/ERA - PaySpan Health . To register call: 1-877-331-7154 or visit
Download Ambetter Quick Reference Guide

Information
Domain:
Source:
Link to this page:
Documents from same domain

MEMBER REIMBURSEMENT MEDICAL CLAIM FORM
ambetter.pshpgeorgia.comMEMBER REIMBURSEMENT MEDICAL CLAIM FORM (For Medical claims only - please complete one form per family member per provider) Instructions You will need your health care provider to assist and supply information in completing this form, including the procedure code(s) and diagnosis code(s).

Peach State Health Plan - Specialty Medication Prior ...
ambetter.pshpgeorgia.comSPECIALTY MEDICATION PRIOR AUTHORIZATION FORM Complete this form and send information to Peach State Health Plan, Pharmacy Department fax at 1-866-374-1579 For questions, please call 800-514-0083 option 2 ACARIA Ship to: Patient Other . OR Dispense from Office, Hospital, or Outpatient Center Stock PATIENT INFORMATION . Patient Name: Address:

2021 Prescription Drug List - ambetter.pshpgeorgia.com
ambetter.pshpgeorgia.com2021 Prescription Drug List Effective January 1, 2021 . Formulary Introduction FORMULARY . The Ambetter from Peach State Health Plan Formulary, or Preferred Drug List, is a guide to available brand and ... Please note, the Formulary is not meant to be a complete list of the drugs covered under your prescription benefit.
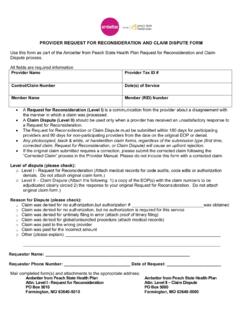
Georgia - Provider Request for Reconsideration and Claim ...
ambetter.pshpgeorgia.comcorrected claim, Request for Reconsideration, or Claim Dispute) will cause an upfront rejection. If the original claim submitted requires a correction, please submit the corrected claim following the “Corrected Claim” process in the Provider Manual. Please do not include this form with a corrected claim. Level of dispute (please check):
Related documents

Florida Medicaid
ahca.myflorida.comAHCA, as a guide for authorizations performed at the first review level. If services cannot be approved at the first level review, the QIO’s physician peer reviewer will determine medical necessity using his or her clinical judgment, acceptable standards of care, state and federal laws, and AHCA’s medical necessity definition.

AMBETTER- PROVIDER BILLING GUIDE 010515
ambetter.superiorhealthplan.comAll required fields are completed on an original CMS 1500 Claim Form, CMS 1450 (UB-04) Claim Form, EDI electronic claim format, or claims submitted on our Secure Provider Portal, individually or batch. All claim submissions will be subject to 5010 validation procedures based on CMS Industry Standards.

NC Medicaid: State Plan Personal Care Services (PCS), 3L.
files.nc.govNC Medicaid shall deny the claim for coverage for an NCHC beneficiary who does not meet the criteria within Section 3.0 of this policy. Only services included under the NCHC State Plan and the NC Medicaid clinical coverage policies, service definitions, or billing codes are covered for an NCHC beneficiary.
Provider Manual
provider.carefirst.comNASCO claim submission Member Identification Card Quick Reference Guide Front of card Back of card Product information Out‑of‑area coverage (BlueCard) CareFirst BlueCross BlueShield is the shared business name of CareFirst of Maryland, Inc. and Group Hospitalization and Medical Services, Inc. CareFirst of Maryland, Inc.,

AmeriHealth Caritas Louisiana Provider Manual
www.amerihealthcaritasla.comJul 01, 2021 · Provider Manual was created as a guide to assist you and your office staff with pro viding ser ice to our m embers, your pat i nts. A a co d io of providing services to AmeriHealth Caritas Louisiana members, providers agree to comply with the provisions in this manual. No content found in this publication or in the
IMPORTANT NOTICE DUE TO COVID 19 EMERGENCY …
www.bcbst.comA. How to File a Claim 1. Filing Electronic Claims (Required Method) 2. Filing Paper Claims 3. Tips for Completing CMS-1500 and CMS -1450 Claim Forms 4. CMS-1500 Health Insurance Claim Form 5. Completing CMS-1500 Claim Form 6. Staff Supervision Requirements for Delegated Services 7. Locum Tenens Policy 8. CMS-1450 Facility Claim Form 9.
NV Billing General
www.medicaid.nv.govNov 17, 2020 · services (i.e., financial and clinical data). Nevada Medicaid requires providers to retain medical records for a minimum of six years from the date of payment. Upon request, records must be provided free of charge to a designated Medicaid agency, the Secretary of Health and Human Services or Nevada’s Medicaid Fraud ontrol Unit.
Provider and Billing Manual - Peach State Health Plan
www.pshpgeorgia.comAllwell is designed to achieve four main objectives: Full partnership between the member, their physician and their Allwell Case Manager Integrated case management (medical, social, behavioral health, and pharmacy)