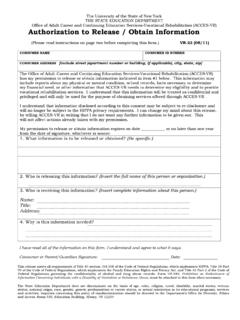
Information Release Authorization
Information Release Authorization . Name: _____ Print full name . The Office of Adult Career and Continuing Education Services (ACCES-VR) has my permission to release or obtain information from agencies [including the Client Assistance program (CAP)], individuals, or employers as are concerned with my vocational rehabilitation. This information
Download Information Release Authorization

Information
Domain:
Source:
Link to this page:
Documents from same domain

UNITING KEY ADULT SERVICE AREAS
www.acces.nysed.govThe State Education Department does not discriminate on the basis of age, color, religion, creed, disability, marital status, veteran status, national origin, race,
PLEASE use this form to obtain school records. …
www.acces.nysed.govRequired Signature of Person Re The University of the State of New York THE STATE EDUCATION DEPARTMENT High School Equivalency (HSE) Office 89 Washington Avenue, EBA 460, Albany, New York 12234
ATTACHMENT R: Application for the New ... - …
www.acces.nysed.govThe University of the State of New York THE STATE EDUCATION DEPARTMENT High School Equivalency (HSE) Office 89 Washington Avenue, EBA 460, …

This application must be mailed to the local test …
www.acces.nysed.govATTACHMENT A The University of the State of New York THE STATE EDUCATION DEPARTMENT APPLICATION FOR . High School Equivalency (HSE) Office . …

THE STATE EDUCATION DEPARTMENT The …
www.acces.nysed.govThe University of the State of New York THE STATE EDUCATION DEPARTMENT T-TAF FORM High School Equivalency (HSE) Office (518) 474-5906 REFERRAL FORM FOR NEW YORK STATE TASC™ TEST APPLICANTS ENROLLED IN AN APPROVED ALTERNATIVE HIGH

VERIFICATION FORM FOR NEW YORK STATE …
www.acces.nysed.govATTACHMENT B To be Completed by School Official The University of the State of New York . THE STATE EDUCATION DEPARTMENT . High School Equivalency (HSE) Office
(ACCES-VR) Application for VR Services
www.acces.nysed.govAre you disabled because of a work-related injury? Do you use any assistive devices or aids? Do you have a NYS driver’s license? Do you have a driver’s license from a state other than New York?
The University of the State of New York
www.acces.nysed.govThe University of the State of New York THE STATE EDUCATION DEPARTMENT Office of Adult Career and Continuing Education …
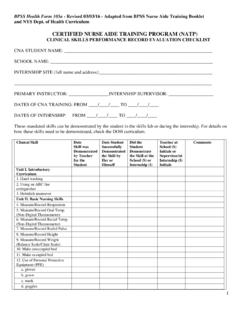
CERTIFIED NURSE AIDE TRAINING PROGRAM …
www.acces.nysed.govcertified nurse aide training program (natp) clinical skills performance record evaluation checklist . ... date clinical skills test p/f written/oral test p/f 1. st:

On-the-Job Training Program - NYS Education Department
www.acces.nysed.govProgram: On-the-Job Training (OJT) is a program by which ACCES-VR can reimburse a new employee’s salary for a mutually agreed upon length of time, contingent on the complexity of the job and the length of training time needed. The expected outcome is permanent employment.
Related documents

CONSENT FOR SURGERY / OPERATION / PROCEDURE(S) …
paloshillssc.comthe matters above. I represent that (a) I have the full right to consent to the matters above; (b) I agree to release, indemnify, and hold harmless the surgery center, its employees, agents, medical staff, partners, and affiliates from any liability or cost arising out of my lack of adequate authority to provide the consent set forth herein. 19.
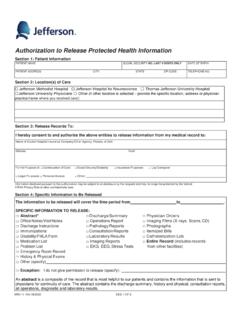
Authorization to Release Protected Health Information
hospitals.jefferson.eduVerbal Consent (If the patient is physically unable to provide a signature. A verbal consent may be revoked by a verbal statement verified in writing by two witnesses.) I witness that the patient was physically unable to provide a signature, but that he/she understood the nature of this release and freely gave his/her oral authorization. Witness

OCA Official Form No.: 960 AUTHORIZATION FOR RELEASE …
nycourts.gov4. I understand that signing this authorization is voluntary. My treatment, payment, enrollment in a health plan, or eligibility for benefits will not be conditioned upon my authorization of this disclosure. 5. Information disclosed under this authorization might be redisclosed by the recipient (except as notedabove in Item ), and this2

Request for Police Certificates/Clearances and ...
www.canada.caAuthorization for Release of Information To Police or Relevant Authorities: Canada Immigration requires the person named below to obtain an original police certificate for every country where he or she has lived for six months or longer since the age of 18. The
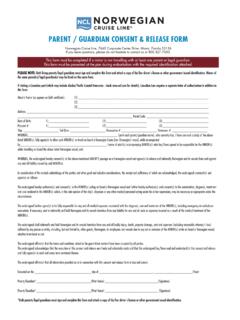
PARENT / GUARDIAN CONSENT & RELEASE FORM
www.ncl.comThe undersigned hereby authorize(s) and consent(s) to the MINOR(s) sailing on board a Norwegian vessel and further hereby authorize(s) and consent(s) to the examination, diagnosis, treatment and care rendered to the MINOR(s) which, in the sole opinion of the ship’s physician or any other medical personnel acting under his or her supervision ...

AUTHORIZATION FOR RELEASE OF PROTECTED OR …
www.partners.org• This authorization will automatically expire 6 months from the date signed unless otherwise specified: • My questions about this authorization form have been answered Patient’s Signature: Date: Print Name: When patient is a minor, or is not competent to give consent, the signature of a parent, guardian, or other legal