
REQUEST FOR VERIFICATION CASE NAME: CASE …
AUTHORIZATION FOR RELEASE OF INFORMATION **OPTIONAL FORM** If you cannot get the proof you need, we may be able to get it for you. Fill out this form and send it …
Download REQUEST FOR VERIFICATION CASE NAME: CASE …

Information
Domain:
Source:
Link to this page:
Documents from same domain

STATEMENT ACKNOWLEDGING REQUIREMENT …
www.cdss.ca.govLIC 9108 (3/05) PAGE 2 OF 2 SIGNATURE DATE WHERE TO CALL IN AND SEND THE WRITTEN ABUSE REPORT Reports of suspected child abuse or neglect must be made to any police department or sheriff's

IN-HOME SUPPORTIVE SERVICES (IHSS) PROGRAM …
www.cdss.ca.govin-home supportive services (ihss) program health care certification form note: the ihss worker may contact you for additional information or to

IMPORTANT INFORMATION FOR PROSPECTIVE …
www.cdss.ca.govstate of california - health and human services agency california department of social services important information for prospective providers about the

Important Information for the In-Home …
www.cdss.ca.govTEMP 3001 (11/15) PAGE 1 of 7 STATE OF CALIFORNIA – HEALTH AND HUMAN SERVICES AGENCY CALIFORNIA DEPARTMENT OF SOCIAL SERVICES Important Information for the

LICENSE APPLICATION AND INSTRUCTIONS FOR …
www.cdss.ca.govLICENSE APPLICATION AND INSTRUCTIONS FOR FAMILY CHILD CARE HOMES This contains instructions needed to file an application for a Family Child Care Home license, and to gain access to

REQUEST FOR LIVE SCAN SERVICE - COMMUNITY …
www.cdss.ca.govguidelines for community care licensing (ccld) applicants who use a live scan site (ccld ordoj site) for fingerprinting instructions for the lic 9163

STATE OF CALIFORNIA - HEALTH AND HUMAN …
www.cdss.ca.govstate of california - health and human services agency california department of social services community care licensing division lic 9214 (6/16) page 2 of 2

STATE OF CALIFORNIA – HEALTH AND HUMAN …
www.cdss.ca.govSTATE OF CALIFORNIA – HEALTH AND HUMAN SERVICES AGENCY CALIFORNIA DEPARTMENT OF SOCIAL SERVICES . APPLICATION FOR SOCIAL SERVICES . To the Applicant: All sections of this form must be completed.

STATEMENT ACKNOWLEDGING REQUIREMENT …
www.cdss.ca.govsoc 341a (3/15) statement acknowledging requirement to report suspected abuse of dependent adults and elders name position facility note: retain in employee/ volunteer file

STATE OF CALIFORNIA – HEALTH AND HUMAN …
www.cdss.ca.govREPORT OF SUSPECTED DEPENDENT ADULT/ELDER FINANCIAL ABUSE FINANCIAL INSTITUTIONS ONLY GENERAL INSTRUCTIONS PURPOSE OF THE FORM This form is to be used by officers and employees of financial institutions (“mandated reporter(s)”) to report suspected
Related documents

CLAIM FORM - PART B TO BE FILLED BY THE …
emeditek.co.inUse dd-mm-yy format Use hh-mm format GUIDANCE FOR FILLING CLAIM FORM - PART B (To be filled in by the hospital) SECTION A- …

APPLICATION FORM - Aavin
www.aavinmilk.comAPPLICATION FORM (for the posts below Manager Cadre) Post applied for Advertisement No. and Date 1. Name of the Candidate ( in BLOCK LETTERS)

Lead Acid Battery Wet, Filled with Acid 04-30-13
www.eastpenncanada.comPAGE 1 OF 8 East Penn Manufacturing Co., Inc. MATERIAL SAFETY DATA SHEET LEAD ACID BATTERY WET, FILLED WITH ACID

CASHLESS CLAIM FORM Toll Free No. 1800-345 …
www.geninsindia.comGUIDANCE FOR FILLING CLAIM FORM - PART B (To be filled in by the hospital) DATA ELEMENT DESCRIPTION FORMAT a) Name of the hospital: b) Hospital ID

Form No. 2 - Embassy of India Kuwait
www.indembkwt.orgForm No. 2 Page 1 of 3. APPLICATION FORM FOR MISCELLANEOUS SERVICES ON INDIAN PASSPORT . For (a) Renewal (b) Change of Address (c) …
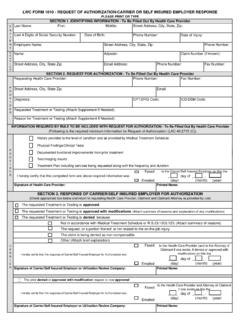
PLEASE PRINT OR TYPE SECTION 1. IDENTIFYING …
www.laworks.netFaxed Emailed Faxed Emailed Faxed Emailed C A R R I E R P R O V Appeal of Suspension to Medical Services Section by Health Care Provider I hereby certify that this First Request and accompanying Form 1010A was _____ day of _____ , _____

CLAIM FORM - PART A' to 'CLAIM FORM FOR …
www.mdindiaonline.comclaim form - part a' to 'claim form for health insurance policies other than travel and personal accident - part a to be filled by the insured

Required NYS School Health Examination Form
www.p12.nysed.govrev. 5/4/2018 page 1 of 2 required nys school health examination form to be completed in entirety by private health care provider or school medical director