WORKERS COMPENSATION APPLICATION DATE …
WORKERS COMPENSATION APPLICATION DATE (MM/DD/YYYY) PARTNERS, OFFICERS, RELATIVES ( Must be employed by business operations) TO BE INCLUDED OR EXCLUDED (Remuneration/Payroll to be included must be part of rating information section.) Exclusions in Missouri must meet the requirements of Section 287.090 RSMo.
Download WORKERS COMPENSATION APPLICATION DATE …

Information
Domain:
Source:
Link to this page:
Documents from same domain
AGENCY CUSTOMER ID: COMMERCIAL GENERAL …
acords.comattach to acord 125 agency customer id: effective date carrier naic code policy number applicant / first named insured agency 4. retroactive date: 3. number of employees covered by employee benefits plans:
WORKERS COMPENSATION APPLICATION DATE …
acords.com16.are physicals required after offers of employment are made? acord 130 (2013/09) 15.are athletic teams sponsored? 13.any employees with physical handicaps?

UMBRELLA / EXCESS SECTION DATE (MM/DD/YYYY)
acords.comACORD 131 (2013/12) $ $ VOLUNTARY Attach to ACORD 125 IMPORTANT - If CLAIMS MADE is checked in the POLICY INFORMATION section below, this is an application for a claims-made policy.
EVIDENCE OF COMMERCIAL PROPERTY INSURANCE
acords.comEVIDENCE OF COMMERCIAL PROPERTY INSURANCE REMARKS - Including Special Conditions (Use only if more space is required) ACORD 28 (2014/01) Page 2 of 2

CANCELLATION REQUEST / POLICY RELEASE
acords.cominsured mortgagee company loss payee lienholder finance company name and address request / release distribution producer's signature date reason for cancellation
AGENCY CUSTOMER ID: BUSINESS OWNERS SECTION
acords.comREMARKS (ACORD 101, Additional Remarks Schedule, may be attached if more space is required) ACORD 160 (2014/12) AGENCY CUSTOMER ID: START TIME: END TIME: 24 HOUR OPERATIONS

PROPERTY SECTION DATE (MM/DD/YYYY) - Free …
acords.comded blkt # amount type blkt # amount type mine subsidence coverage (required in il, in, ky and wv) accept coverage reject coverage limit: $ type
ACORD 0080 2013-09
acords.comacord 80 (2013/09) years, at this or any location? any losses, whether or not paid by insurance, during the last $ applicant's initials: y / n if yes, indicate below loss history

EVIDENCE OF PROPERTY INSURANCE - Frequently …
acords.comloan # authorized representative name and address additional interest loss payee mortgagee additional insured remarks (including special conditions)
DWELLING FIRE APPLICATION DATE (MM/DD/YYYY)
acords.comacord 84 (2013/09) explain all "yes" responses unless stated otherwise y / n 1.any other insurance with this company? (list policy numbers) line of business policy number line of business policy number
Related documents
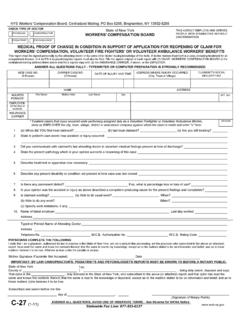
Medical Proof of Change in Condition in Support of ...
www.wcb.ny.govHIPAA NOTICE - In order to adjudicate a workers' compensation claim, WCL 13-a(4)(a) and 12 NYCRR 325-1.3 require health care providers to regularly file medical reports of treatment with the Board and the carrier or employer.

WORKERS COMPENSATION APPLICATION DATE …
ric-ins.comWORKERS COMPENSATION APPLICATION DATE (MM/DD/YYYY) PARTNERS, OFFICERS, RELATIVES ( Must be employed by business operations) TO BE INCLUDED OR EXCLUDED (Remuneration/Payroll to be included must be part of rating information section.) Exclusions in Missouri must meet the requirements of Section 287.090 RSMo. NAME DATE OF BIRTH …

Construction Industry Licensing Board Form # DBPR CILB 18 ...
www.myfloridalicense.comApplication for Change of Status- One Qualified Business to Another Qualified Business . ... Birth Date (MM/DD/YYYY) / / Gender Male Female MAILING ADDRESS ... Have you obtained workers’ compensation insurance or filed for an exemption with the Division of Workers’ Compensation, and if not, do you attest that you will obtain an exemption ...
Hand, Wrist and Forearm Injuries - Government of New York
www.wcb.ny.govJan 01, 2014 · The principles summarized in this section are key to the intended application of the New York State Medical Treatment Guidelines (MTG) and are applicable to all Workers’ Compensation Medical Treatment Guidelines. A.1 Medical Care Medical care and treatment required as a result of a work-related injury should be focused

2643A - Missouri Tax Registration Applicaiton
dor.mo.gov5. Ownership Type. r Sole Proprietor r Partnership r Government r . Trust All ownership types listed below, unless specifically exempted, are required to be registered with the Missouri Secretary of State’s Office (register

Trade Name Instructions - Wyoming
sos.wyo.govThe Application for Registration of Trade Name must be in compliance with Wyoming Statutes 40-2- ... (Workers’ Compensation or Unemployment Insurance) ... (Date – mm/dd/yyyy) •The name must be in use in Wyoming prior to registration. Date:

STATE OF CALIFORNIA DIVISION OF WORKERS' …
www.dir.ca.govStart Date End Date . MM/DD/YYYY MM/DD/YYYY End Date . MM/DD/YYYY MM/DD/YYYY Second Period of Disability: Start Date . 5. Compensation: Compensation was paid: Yes . No Total paid: Weekly rate(s): Date of last payment: MM/DD/YYYY . 6. Has the worker received any unemployment insurance benefits and/or any unemployment compensation

Information & Assistance Unit guide 4
www.dir.ca.govDIVISION OF WORKERS' COMPENSATION WORKERS' COMPENSATION APPEALS BOARD APPLICATION FOR ADJUDICATION OF CLAIM. D . Amended Application Case No. SSN (Numbers Only) Venue choice is based upon (Completion of this section is required) D . County of residence of employee (Labor Code section 5501.5(a)(1) or (d).) D

Application Form for Rent Assist - Province of Manitoba
www.gov.mb.caAPPLICATION FOR RENT ASSIST (for persons not receiving Employment and Income Assistance) This application is available in . alternate formats. upon request. DOCUMENTS THAT MUST BE INCLUDED WITH THIS APPLICATION. You must include a Proof of Income (Option C) for all individuals over the age of 18 who are part of the household.

Social Security Number - Government of New Jersey
www.myleavebenefits.nj.govDS-1 (6/19) 1 Last name First name Middle DSDSDS Internal Code 2 Home Address(Street, Apt #, City, State, ZIP Code) 6 County 3 Mailing Address–if different from home address (Street, Apt #, City, State, ZIP Code)