Transcription of Additional Therapist Credentialing Form - Logon
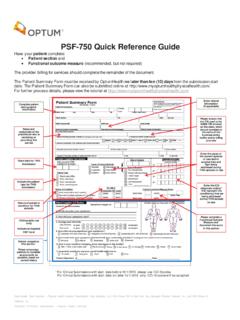
1 Additional Therapist Credentialing form Thank you for informing ACN Group, Inc. (OptumHealth) of an Additional Therapist at your clinic. To begin the Credentialing process, please complete and return this simple, standardized form via fax to (866)459-8101 or via email to This required information is used only for Credentialing and health plan purposes. OptumHealth uses the Council for Affordable Healthcare (CAQH) Universal Provider Datasource (UPD) Web-based Credentialing application. If you already have a complete CAQH application, please ensure that you authorize OptumHealth to access your application. If you do not have a CAQH application, you will receive your ID in the mail.
2 Upon receipt of this letter, register at , complete your application, and authorize OptumHealth to access your application. Please make sure that you upload a copy of the clinic s malpractice insurance declarations page to the CAQH application. Last Name: First Name: Middle Initial: Former Last Name (if applicable): Date of Birth: / / Provider Type: DC PT OT SLP LAC D/N MT ND Social Security #: - - Email: State License #: Licensed State: Medicaid/TPIN#: N/A Medicare #: N/A NPI: Tax ID: Are you registered with CAQH?
3 Yes No If Yes, CAQH ID: Clinic Name: Clinic Street Address: Suite #: City: State: Zip: Clinic Phone #: Clinic Fax #: Mailing Address: Suite#: City: State: Zip: Credentialing Contact Name: Phone # : Fax # : E-mail.