And Disclose
Found 8 free book(s)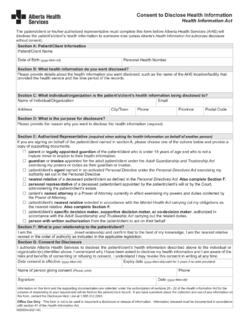
Consent to Disclose Health Information Form
albertahealthservices.caI authorize Alberta Health Services to disclose the patient/client’s health information described above to the individual or : organization(s) identified above. I understand why I have been asked to disclose my health information and I am aware of the risks and benefits of consenting or refusing to consent.

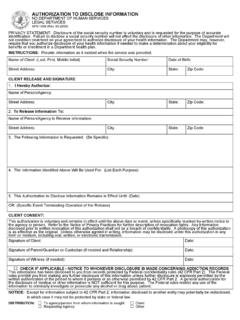
CLAIMANT'S AUTHORIZATION TO DISCLOSE WORKERS' …
www.wcb.ny.govCLAIMANT'S AUTHORIZATION TO DISCLOSE WORKERS' COMPENSATION RECORDS (Pursuant to Workers' Compensation Law Section 110-a) PO Box 5205, Binghamton, NY 13902-5205. l . www.wcb.ny.gov. CLAIMANTS ARE PROHIBITED FROM AUTHORIZING RELEASE OF WORKERS' COMPENSATION INFORMATION TO

Rule 26. Duty to Disclose; General Provisions Governing ...
www.dccourts.gov(D) Time to Disclose Expert Testimony. A party must make these disclosures at the times and in the sequence set forth in the scheduling order issued pursuant to Rule 16(b)(5)(C) and (D). (E) Supplementing the Disclosure. The parties must supplement these disclosures when required under Rule 26(e). (3) [Omitted]. (4) Form of Disclosures. Unless ...

Limited Information - Medicare
www.medicare.govDisclose my personal health information indefinitely Disclose my personal health information for a specified period only beginning: _____(mm/dd/yyyy) and ending: _____(mm/dd/yyyy) 4. Fill in the reason for the disclosure (you may write "at my request"): 5. Fill in the name and address of person or organization to whom you want Medicare to
AUTHORIZATION TO DISCLOSE INFORMATION NORTH …
www.nd.govAuthorization to Disclose Information Form SFN 1059. Individual's full/complete name. If there is a suffix after the name (Sr., Jr.), please provide it in the space along with the last name. Previous name(s) used by the individual. Individual's date of birth. Individual's Social Security Number.

Authorization for Use or Disclosure of Protected Health ...
my.therapysites.comAuthorization and Signature I authorize the release of my confidential protected health information, as described in my directions above. I understand that this authorization is voluntary, that the information to be disclosed is protected
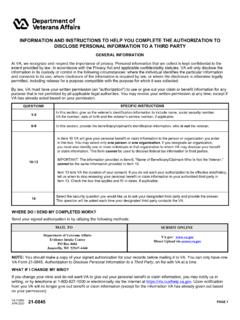
INFORMATION AND INSTRUCTIONS TO HELP YOU …
www.vba.va.gov10. va is authorized to disclose the information specified below to one person or one organization listed below. provide the name and address of the person you have chosen to receive information from va in items 10a and 10b or provide
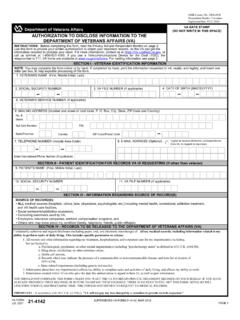
(DO NOT WRITE IN THIS SPACE) AUTHORIZATION TO …
www.vba.va.govauthorization to disclose information to the department of veterans affairs (va) section iii - information regarding source of record(s) va form jul 2021 21-4142€ supersedes va form 21-4142, mar 2018. omb control no. 2900-0858 respondent burden: 5 minutes expiration date: 07/31/2024. page 1. instructions: