Authorization to use and or disclose
Found 8 free book(s)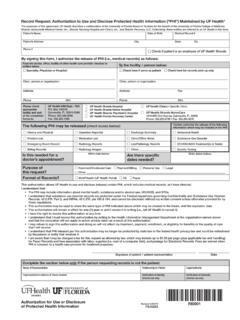
Record Request: Authorization to Use and Disclose ...
ufhealth.orgThis authorization allows UF Health to use and disclose (release) certain PHI, which includes medical records, as I have directed. I understand that: •The PHI may include information about mental health, substance and/or alcohol use, HIV/AIDS, and STDs.

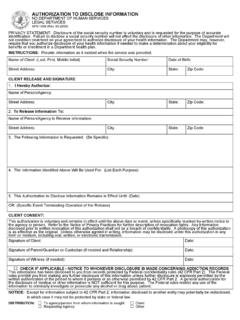
AUTHORIZATION TO DISCLOSE PROTECTED HEALTH …
eforms.comThe authorization provided by use of the form means that the organization, entity or person authorized can disclose, commu-nicate, or send the named individual’s protected health information to the organization, entity or person identified on the form, including through the use of any electronic means. Page 2 of 2

AUTHORIZATION TO DISCLOSE/OBTAIN HEALTH …
hartfordhealthcare.orgauthorization to disclose/obtain health information Subject to the statements printed on the back, I, the undersigned patient or legal representative, hereby authorize the use and disclosure of health information including, if applicable, information …

Authorization for Use or Disclosure of Protected Health ...
my.therapysites.comby law, and the use/disclosure is to be made to conform to my directions. The information that is used and/or disclosed pursuant to this authorization may be re-disclosed by the recipient unless the recipient is covered by state laws that limit the use and/or disclosure of my confidential protected health information.

Authorization to Disclose Information to Disability ...
www.dhs.wisconsin.gov• Authorize the use of a copy (including electronic) or fax of this form for the disclosure of information described above • Understand that there are some circumstances where this information may be disclosed to other parties (see page 2) • May write to DDB and other sources to revoke this authorization at any time (see page 2)

Authorization to Disclose Health Information Form
www.ibx.comInstructions for Completing the Authorization to Disclose Health Information Form If you have any questions, please feel free to call us at the customer service number on your member identification card. Please read the following for help completing page one of the form.
AUTHORIZATION TO DISCLOSE INFORMATION NORTH …
www.nd.govAuthorization to Disclose Information Form SFN 1059. Individual's full/complete name. If there is a suffix after the name (Sr., Jr.), please provide it in the space along with the last name. Previous name(s) used by the individual. Individual's date of birth.
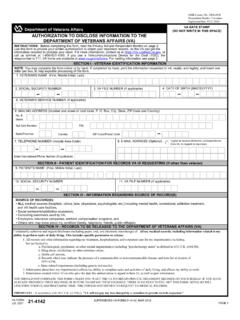
(DO NOT WRITE IN THIS SPACE) AUTHORIZATION TO …
www.vba.va.govUse this form to provide your written authorization to obtain your treatment records, so the VA can get the information required to process your claim. For more information, contact us at . https://iris.custhelp.va.gov, or . call us toll-free at 1-800-827-1000. If you use a Telecommunications Device for the Deaf (TDD), the