Champva claim form
Found 7 free book(s)
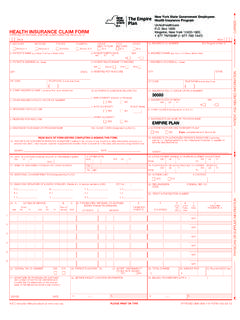
Health Insurance Program HEALTH INSURANCE CLAIM FORM
www.empireplanproviders.com1. medicare medicaid tricare champva group feca other champus health plan blk lung
National Uniform Claim Committee CMS-1500 Claim
www.mdcodewizard.comThe 1500 Health Insurance Claim Form (1500 Claim Form) answers the needs of many health care payers. It is the basic paper claim form prescribed by many payers for claims submitted by physicians,

CMS 1500-Health Insurance Claim Form - USRDS
www.usrds.orgBECAUSE THIS FORM IS USED BY VARIOUS GOVERNMENT AND PRIVATE HEALTH PROGRAMS, SEE SEPARATE INSTRUCTIONS ISSUED BY APPLICABLE PROGRAMS. NOTICE: Any person who knowingly files a statement of claim containing any misrepresentation or any false, incomplete or misleading information may

CHAMPVA Potential Liability Claim VA Health Administration ...
www.va.govIf more space needed, continue in the same format on separate sheet. Attention: After reviewing the following, complete form in its entirety (print or typewritten only) and return.
www.empireplanproviders.com
www.empireplanproviders.comINSURANCE FRAUDS PREVENTION ACT The following statement is printed pursuant to Regulation 95 of the New York State Insurance Department: “Any person who knowingly and with intent to defraud any insurance company or other person files a statement of claim

PATIENT AUTHORIZATION AND CONSENT - insupport.com
www.insupport.comP-BAG-US-00223 EXPIRY February 2020 Page 2 of 3 Fax INSUPPORT: 844-814-0669 Patient Certification for the INSUPPORT Copay Assistance Program (Private or Commercial insurance only) By signing this enrollment form, I certify that I have read, understand and agree to the Terms and Conditions of the INSUPPORT Copay Assistance

YOUR MEDICATIONS - vfwilserviceoffice.com
www.vfwilserviceoffice.comYOUR MEDICATIONS A Handbook for the CHAMPVA Program www.va.gov/hac IMPORTANT PHONE NUMBERS NAME TELEPHONE NUMBER YOUR DOCTOR (PRIMARY CARE) YOUR DOCTOR