Example: quiz answers
Claim Reimbursement
Found 4 free book(s)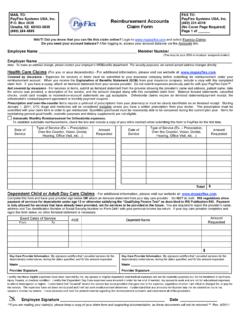
MAIL TO: FAX TO: Reimbursement Accounts Claim Form
www.payflex.comMAIL TO: PayFlex Systems USA, Inc. P.O. Box 3039 Omaha, NE 68103-3039 (800) 284-4885 Reimbursement Accounts Claim Form FAX TO: PayFlex Systems USA, Inc.

Billing and Reimbursement Guideline: UB 04 General Claim ...
www.nhpri.orgVersion History Original Publish Date: 9/1/2010 Revision Date (s): 9/1/2013 Format change, language added regarding Bill Type 33X phase out

Claim for Reimbursement Form - Flex Benefit Administrators
www.fbaflex.comFLEX BENEFIT ADMINISTRATORS www.fbaflex.com claims@fbaflex.com PO BOX 800518 HOUSTON, TX 77280-0518 PHONE (713) 460-FLEX (3539) FAX (713) 460-3550 Claim for Reimbursement Form …

State of Connecticut Dependent Care Assistance Program ...
www.ctpbs.comMAIL OR FAX COMPLETED FORM TO: Progressive Benefit Solutions, LLC (PBS), 14 Business park Drive #8, Branford, CT 06405 FAX: (203) 974-4890 Phone: 1-866-906-8023 State of Connecticut EMPLOYEE NAME SOCIAL SECURITY NUMBER EMPLOYEE NUMBER DAYTIME PHONE NO.