Email Letter Of Medical Necessity
Found 8 free book(s)
Ambetter Provider Claims & Payments FAQ
ambetter-es.coordinatedcarehealth.com*Ensure the denial letter is included the corrected claim. If a paper claim is filed it must be sent on ... requires a review of the claim with medical records to verify medical necessity to prevent incorrect billing. ... Email an image of the check to your Provider Network Specialist for …

Health Savings Account eligible expenses
www.premera.comcan be used for medical reasons or general health purposes are considered “dual purpose”and are eligible only with a doctor’s directive or letter of medical necessity. *Some health insurance premiums are considered eligible expenses. Call 800-941-6121 for more information. Examples include: COBRA premiums,
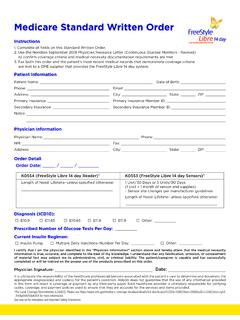
Medicare Standard Written Order - MyFreeStyle
provider.myfreestyle.com2. Use the Noridian September 2018 Physician Resource Letter (Continuous Glucose Monitors - Revised) to confi rm coverage criteria and medical necessity documentation requirements are met. 3. Fax both this order and the patient’s most recent medical records that demonstrate coverage criteria

Idaho Medicaid DME Prior Authorization Form
www.idmedicaid.comDMEPOS PA Policy and Medical Criteria Manual and Supplier Handbook. ☐Physician’s order, Letter of Medical Necessity, and all required documentation is included. ☐Supplier understands request for services does not guarantee payment. ☐Supplier understands PA requests must be complete and valid or it will be denied due to incomplete ...
Provider Appeal Form - bcidaho.com
providers.bcidaho.comPlease include the email contact number assigned in your initial inquiry response. Contact #: Please also include your Prior Authorization Reference number if applicable. Reference #: This form should only be used for reasons documented in your provider contract, such as: • Medical Necessity • Investigational • Clinical Editing
Member Appeal Request
www.premera.comMedical necessity of the service Cancellation of my policy or eligibility . Other (please specify): Please complete the following if related to a medical service: Provider: (doctor’s name, hospital, laboratory) Address: City/State: ZIP code: Date of service: MM/DD/YY Claim #: (Include additional claim numbers in section D.) Total charge:

Louisiana State Board of Nursing
www.lsbn.state.la.usPrior to engaging in medical diagnosis and management as an Advanced Practice Registered Nurse (APRN), including writing orders and/or prescriptions, the APRN must obtain a letter of approval issued to the APRN from the Louisiana State Board of

cpt codes for Applied behavior Analysis
www.abainternational.orgKnow payor policies and requirements for medical necessity and coverage of ABA services, as well as the terms for modification of agreements. • Compliance with contract provisions and payor requirements regarding claims documentation is essential, especially in light of recent billing fraud cases and heightened scrutiny of billing for ABA ...