Employee Change Application
Found 8 free book(s)
Enrollment / Change Application
www.bluecrossnc.comApplication Continued on Next Page. Page. 2. of. 8. Employee Name: B. If Enrolling Due to a Qualifying Life Event C. If Making a Change from Previous Enrollment. Marriage Exhaustion of COBRA Continuation. Divorce Loss of dependent status. Death Reduction in hours. Termination of other coverage Termination of employment. Offered plan is no ...

Health Benefits Application - New York City
www1.nyc.govI certify that the above employee/retiree is eligible for the New York City Health Benefits Program (HBP) and that dependent documentation has been verified in accordance with HBP ... Application/Change Form. Section J: If you are a NEW retiree (even if you are waiving City coverage), your payroll/personnel office must complete this section.

Application to Change Contractor Business Name ($100 Fee ...
www.cslb.ca.govApplication to Change Contractor Business Name ($100 Fee, non-refundable) ... employee (RME) cannot sign this form. ... and representations made or provided by me in this application, including all supplementary statements attached hereto, are true and correct, and that I have reviewed the entire contents of this application.

Group Enrollment Application Change Form - BCBSTX
www.bcbstx.comenrollment application/change form instructions Changes in state or federal law or regulations, or interpretations thereof, may change the terms and conditions of coverage. Check all the boxes that apply to indicate if you are a new enrollee or if you are requesting a …
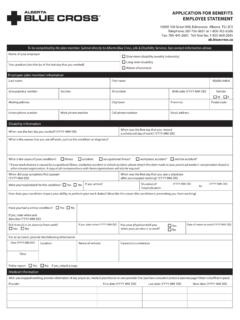
APPLICATION FOR BENEFITS EMPLOYEE STATEMENT
www.ab.bluecross.caAPPLICATION FOR BENEFITS EMPLOYEE STATEMENT 10009 108 Street NW, Edmonton, Alberta T5J 3C5 Telephone: 587-756-8631 or 1-800-763-6206 ... Last date of change (YYYY-MM-DD) Current dosage Frequency Medical history List any other health related condition that you may have at this time

Application Form for Change in Mapping of Employee …
portal.amfiindia.com3. Application form for registration as individual ARN holder along with requisite documents and fees (required in case of option 1 above) 4. The duly signed certificate from the Newly mapped ARN Holder as below (required in case of option 2 above) 5. Letter issued by the New Employer for mapping of EUIN to the ARN of the New Employer, as per the

www.dos.ny.gov Employee Statement and Security Guard ...
dos.ny.govEmployee Statement and Security Guard Application Read ALL instructions carefully before completing the application. Incomplete forms will be returned. Any omission, inaccuracy or failure to make full disclosure may be deemed sufficient reason to deny a registration or may result in the suspension or revocation of an issued registration.

STATE OF TENNESSEE GROUP INSURANCE PROGRAM …
www.tn.govenrollment change application State of Tennessee • Department of Finance and Administration • Benefits Administration 312 Rosa L. Parks Avenue, 19th Floor • Nashville, TN 37243 • 800.253.9981 • fax 615.741.8196