Extended health care claim form
Found 8 free book(s)
Affinity Markets Extended Health Care Claim - …
www.coverme.comI certifythat I, my spouse and/or my dependants of minor or major age ("Dependants"), have received all goods or services claimed and that the information provided for this claim is true and complete. I authorize The Manufacturers Life Insurance Company (Manulife Financial) to collect, use, maintain, and disclose personal

Extended Health Care Claim Form - Sun Life Financial
www.sunlife.caPage . 1. of 2 EHC-E-11-10. Extended Health Care . Claim Form. 1 | Information about you – be sure to fully complete this section • Use this form for all

Extended Health Care and Health Spending …
cdn.sunlife.comPage . 1. of 2 EHC-HSA-E-11-10. Extended Health Care and Health. Spending Account Claim Form. If you’re covered under more than one benefits plan, you should consider submitting your claim to the other plan(s) before using your

Extended Health Care and Health Spending …
www.rbc.comPage . 1. of 2 EHC-HSA-14178-E-09-14 (G4809-E) Extended Health Care and Health. Spending Account Claim Form. If you’re covered under more than one benefits plan, you should consider submitting your claim to the other plan(s) before using your

GENERAL CLAIM SUBMISSION FORM (For Drug …
onlineservices.greenshield.ca*no staples please, paper clips only general claim submission form (for drug and extended health claims) section 1 - plan member information green shield canada id number email address surname first name phone number

PEBA EXTENDED HEALTH CARE PLAN EMPLOYEE …
www.peba.gov.sk.caM635D(PEBA-GE)-12/15 Continued (page 2 of 2) Page 2 of 2 YOU MUST COMPLETE BOTH PAGES Great-West Life Healthcare Expenses Statement PART 9 - Submitting Your Claim
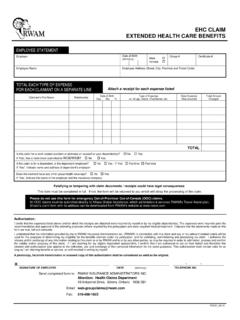
RC001 EHC Claim - RWAM Insurance
www.rwam.comEHC CLAIM EXTENDED HEALTH CARE BENEFITS RC001_09.13 EMPLOYEE STATEMENT Employer Date of Birth (dd/mm/yy) Male Female Group # Certificate # Employee Name Employee Address (Street, City, Province and Postal Code)

CONTINENTAL AMERICAN INSURANCE COMPANY …
www.caicworksite.comCONTINENTAL AMERICAN INSURANCE COMPANY CLAIM FORM Post Office Box 427 Columbia, South Carolina 29202 Phone (800) 433-3036 PART B …
Similar queries
Affinity Markets Extended Health Care Claim, Claim, Extended Health Care Claim Form, Extended Health Care . Claim Form, Form, Extended Health Care and Health Spending, Extended Health Care and Health. Spending Account Claim Form, General claim submission form, Extended health, EXTENDED HEALTH CARE, EMPLOYEE, RC001 EHC Claim, CLAIM EXTENDED HEALTH CARE, CONTINENTAL AMERICAN INSURANCE COMPANY, CONTINENTAL AMERICAN INSURANCE COMPANY CLAIM FORM