Health Benefits Claim Form
Found 6 free book(s)
Mental Health / Substance Abuse Treatment Claim Form
www.valueoptions.comshould be indicated in this block. The Explanation of Benefits from the other insurance carrier needs to be attached to the claim. If the Patient has paid for the charges being submitted on this claim form, please indicate the amount paid in this block. 10. BALANCE DUE - Enter the balance due for services listed on the claim form. 11.

GENERAL CLAIM SUBMISSION FORM (For Drug and Extended ...
onlineservices.greenshield.caof government benefits, the medical information bureau and investigative agency, the City's Employee Health and Rehabilitation Services and my plan sponsor, or other similar persons or entities who have information related to my claim, to release, discuss and exchange information requested by Green Shield Canada, only insofar as any such ...

Dental Claim Form - Health Insurance Plans | Aetna
www.aetna.comform, please indicate a separate fee for each individual service rendered. 2.PREDETERMINATION OF BENEFITS If total charges for this claim are to exceed the minimum Predetermination dollar amount indicated in the employee's Dental Plan Booklet (and treatment is not emergency in nature), Predetermination of Benefits is suggested.

Claim for health care benefits 19132A - Home - DFS
www.desjardinslifeinsurance.com4If your claim is for a dependent, accident-related expenses, out-of-province expenses or an assignment of benefits, please complete the appropriate . section . on the back of the form. 4. Please sign section I and send the form and original receipt to: Desjardins Insurance, C. P. 3950, Lévis (Québec) G6V 8C6
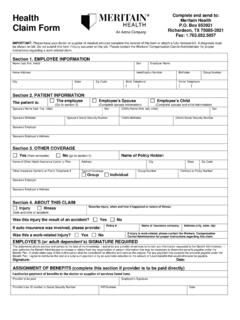
Health Complete and send to: Meritain Health Claim Form ...
www.meritain.comHealth Claim Form Complete and send to: Meritain Health P.O. Box 853921 Richardson, TX 75085-3921 Fax: 1.763.852.5057 IMPORTANT: Please have your doctor or supplier of medical services complete the reverse of this form or attach a fully itemized bill. A diagnosis must be shown on bill. Do not submit this form if injury occurred on the job.

GC-10 - Vision Benefits – Claim Instructions
www.aetna.com4. If you wish to have your benefits for this claim paid directly to your physician or supplier, sign block twenty-eight (28). 5. If you have submitted a request for benefits to another plan, including Medicare, attach a copy of the bills you submitted to the other plan and the explanation of benefits you received from the other plan. 6.