History And Emergency Medical Authorization
Found 4 free book(s)
Health History and Emergency Care Plan, DCF-F-CFS-2345
dcf.wisconsin.govHEALTH HISTORY AND EMERGENCY CARE PLAN . Use of form: This form is required for family and group child care centers and day camps to comply with DCF 250.04(6)(a)1., DCF 251.04(6)(a)6., and DCF 252.41(4)(a)6. of the Wisconsin Administrative Codes. Failure to comply may result in issuance of a noncompliance statement.
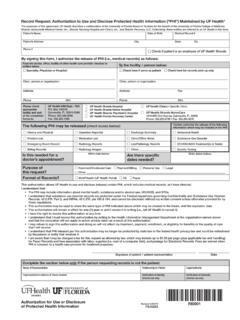
Record Request: Authorization to Use and Disclose ...
ufhealth.orgThis authorization allows UF Health to use and disclose (release) certain PHI, which includes medical records, as I have directed. I understand that: • The PHI may include information about mental health, substance and/or alcohol use, HIV/AIDS, and STDs.

Authorization for Release of Protected Health Information
www.lexmed.comSection 1 – Medical Records Release (Release copies of protected health information) £ Portal £ Mail £ Pick-up £ Fax (to health provider only) £ I request a copy of this authorization *Mail completed form to: Lexington Medical Center Attn: Medical Records, 2720 Sunset Blvd., West Columbia, SC 29169

AUTHORIZATION FOR RELEASE OF MEDICAL INFORMATION
www.nm.orgIf not withdrawn, this authorization is valid for a period of six (6) months from the date of signature and allows release of records past the date signed as long as the authorization is still in effect. Standard record copying fees per 735 ILCS 5/8-2006 may apply. By signing below, I agree to the statements in this authorization form.