Transcription of 38 Foot and Ankle Amputations: Ray Resections
1 1 BACKGROUND Malignant tumors of the foot present a significant and for-midable challenge to the orthopaedic oncologist due to thefoot s unique function and anatomic peculiarities. The foot is uniquely adapted for bipedal motion and assuch is essentially a tripod. The tripod is basically formed bythe first ray, the fifth ray, and the calcaneus and is supportedby the osseous configuration of bones in the midfoot thatform a Roman arch, which in and of itself is inherentlystable. Both bone and soft tissue contribute to the structure andfunction of the foot . Furthermore, the foot is composed ofcompact compartments that are interconnected by nerves andvascular structures.
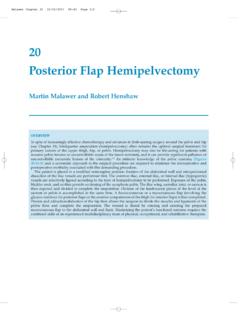
2 Complete resection (wide local excision) ofosseous structures of the foot is difficult because of the inter-ruption of these complex anatomic relationships, which affordstability to the foot , in addition to the interconnected compart-ments. Malignant tumors of bone are rare in the foot and rarerstill in locations distal to the metatarsophalangeal ,5 9 Many of these tumors are treated with amputations. In the senior author s experience of foot and Ankle tumorsin 153 cases, 31 amputations were performed (FIG 1A).Fortunately, tumors distal to the metatarsophalangeal jointcan be treated by amputation through the metatarsopha-langeal joint with minimal disruption to function.
3 The onlyexception is the first ray, which typically bears 50% of theweight with toe-off during each gait cycle. Therefore, preser-vation of as much proximal phalanx as possible is importantto optimize this important Tumors involving the toe or metatarsal bone are tumors affecting the foot , including osteosarcomas,have a low ,2,7 Metastatic tumors of the foot arealso ,11 The most common sites of primary tumors arelung, kidney, and In the senior author s experience of 153 foot and Ankle tu-mors, 73 cases were bony (FIG 1B); of these, 7 cases involvedthe metatarsals (FIG 1C). The indications for ray Resections aretumors involving the toe or metatarsal bone.
4 Benign tumorsmake up the majority of these FIGURE 1 Dshows the distribution of benign versus malig-nant diagnoses. The malignant lesions include metastatic dis-ease, primary bony tumors, and soft tissue The tripod is basically formed by the first ray, the fifth ray,and the calcaneus and is supported by the osseous configura-tion of bones in the midfoot that forms a Roman arch, whichin and of itself is inherently stable. These bones are supported by ligamentous structures aswell as tendons that help preserve the arch and support footfunction. For this reason, Resections of the first and fifth raystypically result in significant alterations in function, especiallythe first ray. The resulting forces after resection of the first rayresult in transfer to the lesser metatarsals, which are illadapted to structurally support the weight of the body, result-ing in transverse metatarsalgia.
5 These structural alterations can be mitigated in part by thejudicious use of orthotics, such as a medial heel wedge totransfer the forces farther lateral or the use of a metatarsal bar,which will more evenly distribute the weight across the lessermetatarsals. Resection of the fifth ray is relatively easily com-pensated for by creating an orthosis that transfers the forcesmedially; thus, a lateral heel wedge is beneficial. Resection of the middle rays results in insignificant loss offunction and acceptable cosmesis. The only net result is nar-rowing of the forefoot, which can be easily compensated forwith shoe HISTORY AND PHYSICALFINDINGS Patients with tumors of the toe or metatarsal present withpain and mass.
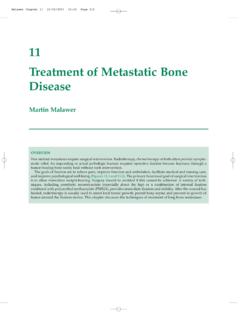
6 The mass may be small and chronic. It may ap-pear with an injury. Physical examination (Table 1) will reveal a tender masslocalized to the toe or metatarsal. There may be associatedswelling. If a sensory nerve overlies the mass, there may AND OTHER STAGING STUDIES Preoperative studies include plain radiographs of the foot ,including anteroposterior, lateral, and oblique views. If theankle joint is involved, then anteroposterior and mortise viewsare obtained. MRI is important to evaluate the amount of involvement ofthe metatarsals to determine the level of amputation. The casein FIGURE 2shows cortical thickening of the secondmetatarsal. The clinical photographs show increased space be-tween the metatarsals.
7 MRI shows the soft tissue lesion was found to be MANAGEMENT The goal of the surgical procedure is to remove the tumorwith adequate margins. A long plantar flap is important for a sturdy end-bearingstump. The bony edges should be smooth and beveled if possible. Myodesis is helpful to pad the end of the stump. Figure 2shows pigmented villonodular synovitis (PVNS) lo-calized to the plantar aspect of the first metatarsal head. Theclinical photographs show the mass. MRI shows the soft tissueinvolvement. Intraoperative photograph shows resection ofthe B. Chou, H. Thomas Temple, Yvette Ho, and Martin M. MalawerFoot and Ankle Amputations: Ray 4/10/09 12:35 PM Page 12 Part 4 ONCOLOGY Section IVLOWER EXTREMITIESABCDFIG 1 of types of amputations for 153 tumors of the foot and Ankle (n 31).
8 Diagnoses of bony tumors of thefoot and Ankle (n 73). of metatarsal tumors (n 7). of bony tumors of the foot and Ankle by diagnosisand site (n 73).ExaminationTechniqueSignificanceInsp ectionEvaluate the lower extremity with Examination of both extremities allows for the patient undressed from the to identify and deep palpation of Evaluates tenderness of the mass; evaluates the mass or area of painwhether the mass is mobile or fixedRange of motionObserve passive and active range Identifies joint involvement with tumorof motion of the foot and Palpate dorsalis pedis and Evaluates vascularity of the extremity and examinationposterior tibia there is tumor involvementNeurologic Evaluate motor strength and sensationEvaluates involvement of muscles and examinationto light nervesTable 1 Physical Examination 4/10/09 12:35 PM Page 2 Chapter 38 foot AND Ankle AMPUTATIONS: RAY RESECTIONS3 ABCDEFGFIG 2 tumors canshow cortical thickening, mimickinga stress fracture.
9 In this case, it wasa benign lesion of the secondmetatarsal. photographshows increased space between themetatarsals from the mass. the amount of soft tissueinvolvement. D, synovitis (PVNS) isusually treated with simpleexcision. This case of PVNS waslocalized to the plantar aspect ofthe first metatarsal head. Clinicalphotographs show the mass. soft tissue photographshows tumor Planning Preoperative planning is crucial for a good outcome. Thepreoperative radiographs and CT and MRI studies are impor-tant to determine the amount of tumor involvement. They alsoshow the extent of soft tissue tumors and may be helpful indistinguishing benign from malignant biopsyresults will determine the level of amputation.
10 The level of amputation is an important part of preoperativeplanning. The length of the residual stump is as important asthe quality of soft tissue. There must be adequate padding ofskin, subcutaneous fat, muscle, and tendons to cover the endof the The patient is placed supine on the operating table. A thightourniquet is placed over adequate cotton padding. A bumpmay be placed proximal to the sciatic notch on the ipsilateralhip to limit external rotation of the extremity during The surgical approach is planned preoperatively. It is impor-tant to maintain as much plantar skin as possible because thisskin is thicker and has specialized columns of plantar fat forweight 4/10/09 12:35 PM Page 34 Part 4 ONCOLOGY Section IVLOWER EXTREMITIESTECH FIG 1 incision location in a metatarsalray resection.