Transcription of A tool to calculate safe nurse staffing levels - EMAP
1 Nursing Practice Keywords: Workforce/ staffing /Skill mix/Nursing care tool Review safe staffing Growing evidence on the link between nurse staffing levels and the quality of care has led to the development of a tool and guidance to calculate safe staffing levels A tool to calculate safe nurse staffing levels In this 5 key he importance of appropriate nurse numbers and skill mix T. points Developing a tool to aid local calculation of safe staffing levels 1 nurse staffing levels , skills and experience are key Examples of the tool in use to providing safe , high-quality Authors Katherine Fenton is chief nurse ; the publication of safe staffing in Adult patient care Ann Casey is a senior nurse ; both at University College Hospitals Foundation Trust.
2 Inpatient Wards in Acute Hospitals (National Institute for Health and Care Excellence, 2014) and the first toolkit endorsed by NICE. 2 An evidence- based tool kit endorsed by NICE. Abstract Fenton K, Casey A (2015) A tool for determining safe nurse staffing estab- helps nurses decide to calculate safe nurse staffing levels . lishments for adult in-patient wards. (Shel- on staffing needs Nursing Times; 111: 3, 12-14. ford Group, 2014). The Safer Nursing Care based on patients'. A guideline from the National Institute for Toolkit (SNCT) for adult care in acute hos- levels of sickness Health and Care Excellence and a NICE- pitals was developed by the Shelford Group and dependency, endorsed tool on safer nursing care allow of 10 leading NHS teaching hospitals, and and links staffing decisions on safe staffing levels to be has been endorsed by NICE.
3 Used alongside levels to quality made at a local level. Decisions must be the NICE (2014) guideline, it enables local indicators based on sound evidence and factoring in patients' individual needs as well as numbers of patients. decision making to be based on sound evi- dence, and gives trusts a platform to work together to the same standards. 3 The tool can be used to support requests The Safer Nursing Care Tool helps The NICE guideline requires trusts to for more nurses on nurses decide on safe nurse staffing for ensure the number of nurses and health- wards acute wards based on patients' level of sickness and dependency.
4 It also includes quality indicators linked to nursing care to care assistants funded to work on the wards nurse staffing establishments is sufficient to provide safe care to each 4 The tool is easy to use, but must be help ensure staffing levels achieve best patient at all times . Trusts must involve applied patient care. The tool is easy to use by nursing staff in drawing up staffing poli- consistently frontline nursing staff, but must be applied correctly and consistently for data to be valid, and to allow benchmarking against cies, and when agreeing the mix of regis- tered nurses and HCAs take into account evidence showing care delivered by regis- 5 The tool gives a baseline for staffing decisions, agreed standards.
5 It should be combined tered nurses gives better outcomes than but the final with nurses' professional judgement and that delivered by unregistered staff assessment account for local factors. (NICE, 2014). requires H. Trusts are also required by NHS England consideration of aving the right number of and the Care Quality Commission to dis- local factors nurses, with the right mix of play the actual number of nursing staff skills and experience, is essen- against those planned for each shift out- tial if organisations are to pro- side all inpatient wards. They must publish vide safe , high-quality care for patients.
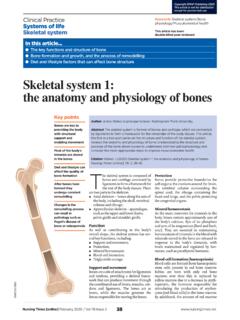
6 Monthly staffing data showing planned However, the needs of hospital patients number of nursing hours against the have changed as demographic changes and number they manage to fill, and carry out a advances in healthcare mean those six-monthly review of their staffing estab- admitted to hospital tend to have more lishments (Department of Health, 2014). complex care needs than in the past. The SNCT is an evidence-based tool that One of the government's responses to helps trusts make staffing decisions that the Francis report into care failings at Mid deliver safe , high-quality care; nurses can The Safer Nursing Care Toolkit allows local Alamy Staffordshire Foundation Trust has led to use it to help work out staffing decision-making based on sound evidence 12 Nursing Times / Vol 111 No 3 / Nursing For articles on nursing management, go to Box 1.
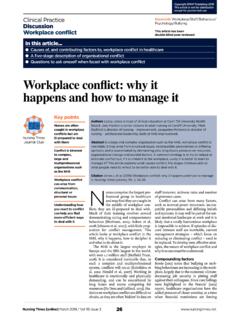
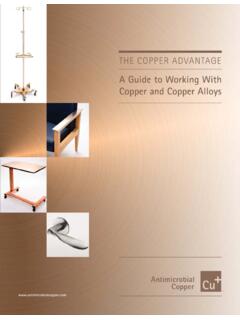
7 Summary of SNCT Classifications Box 2. nurse -sensitive indicators Level Descriptor 0 Patients requiring hospitalisation whose needs are met by normal ward care Official complaints 1(a) Acutely ill patients needing intervention or who are unstable with a greater Received about nursing/midwifery/care potential to deteriorate staff (per 1,000 occupied bed days) in 1(b) Patients who are stable, but depend on nursing care to meet most or all of the areas of: communication, clinical the activities of daily living care, attitude 2 Patients who can be managed within clearly identified and designated beds Drug errors and resources with the required expertise and staffing level or may require Where nursing was the primary cause, transfer to a dedicated Level 2 facility/unit not including near misses per 1,000.
8 3 Patients needing advanced respiratory support and/or therapeutic support occupied bed days of multiple organs Infection Incidence rates of MRSA bacteraemia Multipliers Example per 1,000 occupied bed days and For acute inpatient wards (there are separate multipliers for acute assessment units Clostridium difficile per 1,000 occupied included in the tool) bed days Level 0: 12 patients; Slips, trips and falls Level 1a: 7 patients; Number of slips, trips or falls per 1,000. Level 1b: 8 patients; occupied bed days caused primarily by Level 2: 1 patient; nursing error Level 3: 0 patients Pressure ulcers Total whole-time equivalents Incidence of hospital-acquired pressure (Multipliers include 22% uplift for annual leave etc) ulcers per 1,000 occupied bed days Nutrition Number of patients having had establishments and daily monitoring of nurse -sensitive indicators (NSIs), such nutritional screening per 1,000.
9 Ward staffing needs. The tool can be used to as infection rates, complaints, pressure occupied bed days support requests for more nurses on wards ulcers and falls, so nurses can check Percentage of wards that have and to ensure trusts on finite budgets make staffing levels against quality out- implemented protected mealtimes the best use of qualified staff. comes. policy The tool allows comparison across Why we need a safer staffing tool wards and trusts to help ensure best A growing body of research shows links staffing levels and benchmark against the UK Nursing Database and SNCT to between patient sickness and dependency, agreed national standards.
10 Update the staffing multipliers. As well as workload, staffing and quality of care. Low leading teaching hospitals, many acute staffing levels and a low proportion of reg- Developing and validating the tool trusts are also using it. istered nurses on wards have been linked The SNCT was originally created more to poor patient outcomes, and there is evi- than 10 years ago by Katherine Fenton, How to use the tool dence of increased harm when a registered chief nurse at University College London All participating trusts must collect data nurse cares for eight or more patients Hospitals Foundation Trust, and Hilary using the tool at the same time to ensure during day shifts (NICE, 2014).