Transcription of Alcohol’s Role in Gastrointestinal Tract Disorders
1 Mong the many organ systems that mediate alcohol s effects on the human body and its health,the Gastrointestinal (GI) Tract plays aparticularly important part. Severalprocesses underlie this role. First, theGI Tract is the site of alcohol absorptioninto the bloodstream and, to a lesserextent, of alcohol breakdown and pro-duction. (For more information onalcohol absorption, metabolism, andproduction in the GI Tract , see sidebar,pp. 82 83.) Second, the direct contact ofalcoholic beverages with the mucosa1that lines the upper GI Tract can inducenumerous metabolic and functionalchanges. These alterations may lead tomarked mucosal damage, which canresult in a broad spectrum of acute andchronic diseases, such as acute gastro-intestinal bleeding (from lesions in thestomach or small intestine) and diar-rhea.
2 Third, functional changes andmucosal damage in the gut disturb thedigestion of other nutrients as well astheir assimilation into the body, there-by contributing to the malnutrition andweight loss frequently observed inalcoholics. Fourth, alcohol-inducedmucosal injuries especially in theupper small intestine allow largemolecules, such as endotoxin and otherbacterial toxins, to pass more easilyinto the blood or lymph. These toxicsubstances can have deleterious effectson the liver and other the past three decades, re-searchers have made major progresstoward understanding alcohol s manyacute and chronic effects on GI-tractfunction and structure. This article reviews some of thesefindings, focusing primarily on insightsgained during the past 10 years. (Forextensive reviews of the developments76 ALCOHOLHEALTH& RESEARCHWORLDA lcohol s Role inGastrointestinal TractDisordersCHRISTIANEBODE, , ANDJ.)
3 CHRISTIANBODE, alcohol is consumed, the alcoholic beverages first pass through the varioussegments of the Gastrointestinal (GI) Tract . Accordingly, alcohol may interfere withthe structure as well as the function of GI- Tract segments. For example, alcohol canimpair the function of the muscles separating the esophagus from the stomach,thereby favoring the occurrence of heartburn. Alcohol-induced damage to themucosal lining of the esophagus also increases the risk of esophageal cancer. In thestomach, alcohol interferes with gastric acid secretion and with the activity of themuscles surrounding the stomach. Similarly, alcohol may impair the musclemovement in the small and large intestines, contributing to the diarrhea frequentlyobserved in alcoholics.
4 Moreover, alcohol inhibits the absorption of nutrients in thesmall intestine and increases the transport of toxins across the intestinal walls,effects that may contribute to the development of alcohol-related damage to the liverand other organs. KEY WORDS: ethanol metabolism; AODE (alcohol and other drugeffects); mouth; esophagus; stomach; intestine; gastric mucosa; intestinal mucosa; gastriclesion; gastric acid; Gastrointestinal function; Gastrointestinal absorption; muscle; neoplasticdisease; toxins; free radicals; etiology; literature reviewCHRISTIANEBODE, , is professorand chief of the Section of Physiologyof Nutrition (140), HohenheimUniversity, Stuttgart, CHRISTIANBODE, , is professorof medicine and chief of the Sectionof Gastroenterology, Hepatology andEndocrinology in the Department ofInternal Medicine, Robert-Bosch-Krankenhaus, Stuttgart, a definition of this and other technical terms usedin this article, see the central glossary, pp.
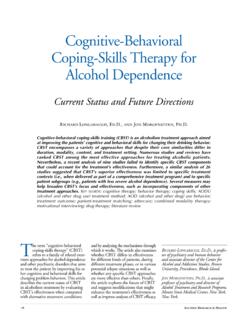
5 93 this field up to the early 1980 s, seeBeazell and Ivy 1940; Bode 1980). THEGI Tract ANOVERVIEWThe GI Tract s functions are to physi-cally and chemically break downingested food, allow the absorption ofnutrients into the bloodstream, andexcrete the waste products GI Tract can be viewed as onecontinuous tube extending from themouth to the anus (figure 1), which issubdivided into different segmentswith specific the mouth, or oral cavity, the teethmechanically grind the food into smallpieces. Moreover, saliva excreted bythe salivary glands initiates the food schemical degradation. From the oralcavity, the food passes through the throat( , pharynx) into the esophagus. Thecoordinated contraction and relaxationof the muscles surrounding the esopha-gus propels the food into the the stomach, the chemical degra-dation of the food continues with thehelp of gastric acid and various diges-tive enzymes.
6 Excessive gastric acidproduction can irritate the mucosa,causing gastric pain, and result in thedevelopment of gastric ulcers. Twobands of muscle fibers ( , sphinc-ters) close off the stomach to the eso-phagus and the intestine. Weakness ofthe sphincter separating the stomachfrom the esophagus allows the stom-ach content to flow back into the eso-phagus. This process, which is calledgastroesophageal reflux, can lead toheartburn as well as inflammation ( ,reflux esophagitis) and even to thedevelopment of ulcers in the lowerpart of the the stomach, the food entersthe small intestine, which is dividedinto three segments: the duodenum,the jejunum, and the ileum. Like theesophagus and stomach, the intestineis surrounded by layers of muscles,the rhythmic movements of whichhelp mix the food mass and push italong the GI Tract .
7 The intestine sinner mucosal surface is covered withsmall projections called villi, whichincrease the intestinal surface area(figure 2). As the food mass movesthrough the small intestine, digestiveenzymes secreted by the intestinalcells complete the chemical degrad-ation of nutrients into simple mole-cules that can be absorbed through theintestinal wall into the finally remains in the intestineare primarily indigestible waste prod-ucts. These products progress into thelarge intestine, where the waste iscompacted and prepared for excretionthrough the anus. Like the small in-testine, the large intestine can bedivided into three segments: the ce-cum; the colon, which constitutesabout 80 percent of the large intes-tine; and the rectum. The followingsections review alcohol s effect on thedifferent regions of the GI THEESOPHAGUSThe oral cavity, pharynx, esophagus,and stomach are exposed to alcoholimmediately after its ingestion.
8 Thus,alcoholic beverages are almost undi-luted when they come in contact withthe mucosa of these structures. It istherefore not surprising that mucosalinjuries ( , lesions) occur quitefrequently in people who drink largeamounts of alcohol abuse damages thesalivary glands and thus interfereswith saliva secretion. In alcoholics thisdamage commonly manifests itself asan enlargement ( , hypertrophy) ofthe parotid gland, although the mecha-nisms leading to this condition areunknown. Moreover, alcoholics maysuffer from inflammation of the tongue( , glossitis) and the mouth ( ,stomatitis). It is unclear, however,whether these changes result frompoor nutrition or reflect alcohol sdirect effect on the mucosa. Finally,chronic alcohol abuse increases theincidence of tooth decay, gum disease,and loss of teeth (Kranzler et al.)
9 1990). Alcohol consumption can affect theesophagus in several ways. For exam-ple, alcohol distinctly impairs esophagealmotility, and even a single drinkingepisode ( , acute alcohol consump-tion) significantly weakens the loweresophageal sphincter. As a result, gastroesophageal reflux may occur,and the esophagus ability to clear therefluxed gastric acid may be of these factors promote theoccurrence of heartburn. Moreover,some alcoholics exhibit an abnormali-ty of esophageal motility known as aVOL. 21, NO. 1, 199777 Gastrointestinal Tract DisordersOral cavityPharynxEsophagusStomach DuodenumJejunumCecumIleumLarge intestine(colon)RectumTeethParotidglandS alivaryglandsTongueAnal canalFigure 1 Schematic representation ofthe human Gastrointestinal Tract . Thesmall intestine comprises the duo-denum, the ileum, and the alcohol amount necessary to cause mucosalinjury varies significantly among individual drinkersand depends, for example, on whether alcoholconsumption occurs on an empty stomach or isaccompanied by a meal.
10 Thus, no clear thresholdexists above which alcohol exerts its adverse , the risk for adverse effects such as tissuedamage generally increases following the consump-tion of more than 2 ounces of alcohol, which corre-sponds to approximately four standard drinks ( , heavy or excessive drinking). nutcracker esophagus, which mim-ics symptoms of coronary heart dis-ease (Bode and Bode 1992).3 Chronic alcohol abuse leads to anincreased incidence not only of heart-burn but also of esophageal mucosalinflammation ( , esophagitis) andother injuries that may induce mucosaldefects ( , esophagitis with or with-out erosions). In addition, alcoholicsmake up a significant proportion ofpatients with Barrett s esophagus. Thiscondition, which occurs in 10 to 20percent of patients with symptomaticgastroesophageal reflux disease(Wienbeck and Berges 1985), is char-acterized by changes in the cell layerlining the esophagus ( , the epitheli-um) that lead to abnormal acid produc-tion.