Transcription of AMERICAN ACADEMY OF PEDIATRICS
1 AMERICAN ACADEMY OF PEDIATRICSTask Force on infant Sleep Position and sudden infant death SyndromeChanging Concepts of sudden infant death syndrome : Implications forInfant Sleeping Environment and Sleep PositionABSTRACT. The AMERICAN ACADEMY of PEDIATRICS hasrecommended since 1992 that infants be placed to sleepon their backs to reduce the risk of sudden infant deathsyndrome (SIDS). Since that time, the frequency of pronesleeping has decreased from>70% to;20% of US in-fants, and the SIDS rate has decreased by>40%. How-ever, SIDS remains the highest cause of infant deathbeyond the neonatal period, and there are still severalpotentially modifiable risk factors. Although some ofthese factors have been known for many years (eg, ma-ternal smoking), the importance of other hazards, such assoft bedding and covered airways, has been demon-strated only recently. The present statement is intendedto review the evidence about prone sleeping and otherrisk factors and to make recommendations about strate-gies that may be effective for further reducing the risk ofSIDS.
2 This statement is intended to consolidate and sup-plant previous statements made by this Task SIDS, sudden infant death infant death syndrome (SIDS) is a dis-ease of unknown cause. Despite recent de-creases in the incidence of SIDS, SIDS is stillresponsible for more infant deaths in the UnitedStates than any other cause of death during infancybeyond the neonatal is defined as: The sudden death of an infant under 1 year ofage, which remains unexplained after a thoroughcase investigation, including performance of a com-plete autopsy, examination of the death scene, andreview of the clinical history. 2 The occurrence of SIDS is rare during the firstmonth of life, increases to a peak between 2 and 4months old, and then declines. The following havebeen consistently identified across studies as inde-pendent risk factors for SIDS: prone sleep position,sleeping on a soft surface, maternal smoking duringpregnancy, overheating, late or no prenatal care,young maternal age, prematurity and/or low birthweight, and male 11 Blacks and AMERICAN Indi-ans have consistently higher rates, 2 to 3 times thenational average.
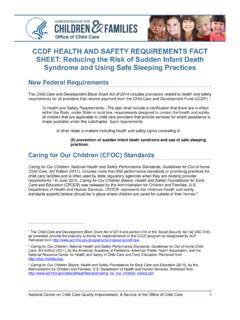
3 The risk factors with the greatestpotential for modification include prone sleep posi-tion, sleeping on a soft surface, maternal smoking,and overheating. National campaigns aimed at re-ducing prone sleeping have resulted in a dramaticdecrease in the incidence of SIDS in the United States(Fig 1) and numerous other 17A Back toSleep campaign was initiated in the United States in1994, as a joint effort of the US Public Health Service,the AMERICAN ACADEMY of PEDIATRICS , the SIDS Alli-ance, and the Association of SIDS and infant Mortal-ity Programs (800-505-CRIB). Despite the success ofthe current campaign, several modifiable risk factorsremain that require increased attention. The pur-poses of this statement are to reemphasize the im-portance of infant positioning for sleep as an effec-tive modifiable risk factor for SIDS, to focusincreased attention on other modifiable environmen-tal factors, to describe complications that may havearisen from modifying risk factors, and to make rec-ommendations about other strategies that may beeffective for further reducing the risk of RISK FACTORSP rone SleepingProne sleeping has been recognized as a major riskfactor for SIDS, with odds ratios ranging from in various well designed epidemiologic ,14,18 21 The plausibility of a causal associationbetween prone sleep positioning and SIDS is mademost compelling by the observation that in countries,including the United States, in which campaigns toreduce the prevalence of prone sleeping have beensuccessful.
4 Dramatic decreases in the SIDS rates haveoccurred. The association is further strengthened byobservations that in cultures in which prone sleepingis rare, SIDS rates historically have been very ,23In addition, several studies have documented thatthe statistical relationship between prone positioningand SIDS often strengthens when corrections aremade for confounding ,24,25 The original 1992 sleeping position recommenda-tion from the AMERICAN ACADEMY of PEDIATRICS iden-tified any nonprone position (ie, side or supine) asbeing optimum for reducing SIDS from England11and New Zealand27haveshown that side sleeping has a slightly higher riskthan the supine position, although the side-sleepingposition still seems to be considerably safer thanprone. The higher risk for SIDS among infants placedon their sides may relate to the relative instability ofthis position. Although infants placed on their sidesusually roll to their backs, the risk of rolling to theprone position from the side is significantly greaterthan rolling to the prone position from the ,12,28 Strategies to decrease prone sleeping in the UnitedThe recommendations in this statement do not indicate an exclusive courseof treatment or serve as a standard of medical care.
5 Variations, taking intoaccount individual circumstances, may be (ISSN 0031 4005). Copyright 2000 by the AMERICAN Acad-emy of Vol. 105 No. 3 March 2000 by guest on November 8, from States have included the following: 1) disseminatinginformation to hospital nurseries and physicians, 2)targeting child care education programs, and 3) ini-tiating public media campaigns. Although somecountries have almost abolished prone sleeping,15,29,30;20% of US infants continue to sleep prone at thehighest risk age range for concern is thatblack infants are twice as likely to be placed prone aswhite infants. In addition, nearly 20% of caregiversapparently switch from placing infants in the non-prone to prone sleep position between 1 and 3months old, the peak age range for ,32 Also,although parents may know of the recommendation,many other child caregivers, such as child care centerworkers, do is also some evidence thatinfants who are accustomed to sleeping supine are atparticularly high risk for SIDS when they subse-quently are placed in a prone position for 36 Soft Sleep Surfaces and Loose BeddingPolystyrene bead-filled pillows were among thefirst soft sleep surfaces identified as contributing tothe deaths of young infants37and subsequently wereremoved from the market following action by the USConsumer Product Safety Commission.
6 Additionalepidemiologic studies identified other soft surfaces,such as pillows, quilts, comforters, sheepskins, andporous mattresses, as a significant risk factor, partic-ularly when placed under the sleeping ,25,38 42 Several reports described that in a significant num-ber of SIDS cases, the heads of the infants, includingsome infants who slept supine, were covered byloose bedding. Many of these studies found loosebedding to be an epidemiologic risk factor ,30,36,38,40,43,44 OverheatingThere is some evidence that the risk of SIDS isassociated with the amount of clothing or blanketson an infant , the room temperature, and the seasonof the ,45 48 The increased risk associated withoverheating is particularly evident when infantssleep prone6but is less clear when they sleep is unclear whether the relationship to clothing andclimate is an independent factor or merely a reflec-tion of the use of more clothing, quilts, and otherpotentially asphyxiating objects in the sleeping envi-ronment during cold weather.
7 The SIDS statisticsalways have shown a distinct seasonality, withhigher rates recorded during winter months. It maybe that the seasonality reflects increased infections,which also are known to be more frequent duringcold weather. A significant decrease has been ob-served in the seasonal association of SIDS as pronesleeping has decreased and SIDS rates have de-creased, thus suggesting an interaction among envi-ronmental smoking during pregnancy has emergedas a major risk factor in almost every epidemiologicstudy of ,10,49,50No intervention studies havedocumented a decrease in SIDS associated with adecrease in maternal smoking, although changingsuch behavior has been far more difficult to accom-plish than changing infant sleep position. Smoke inthe infant s environment after birth has emerged as aseparate risk factor in a few studies,10,51althoughseparating this variable from maternal smoking be-fore birth is rate in the United States (line) from National Center for Health Statistics (NCHS) data and prone-positioning rate fromNational Institute for Child Health and Human Development (NICHD) surveys (bars).
8 The AMERICAN ACADEMY of PEDIATRICS (AAP)recommendation was made at the April 1992 Spring Meeting and was published in June Back to Sleep campaign was begunin ACADEMY OF PEDIATRICS651 by guest on November 8, from Bed SharingThere are some reports of infants being suffocatedby overlying by an adult, particularly when the adultis in an unnaturally depressed state of consciousness,such as from alcohol or mind-altering drugs. Co-sleeping on sofas has emerged as a major risk factorin 1 study (Peter J. Fleming, Department for ChildHealth, Bristol, UK, unpublished data presented at ameeting convened by US Consumer Product SafetyCommission, Bethesda, MD, December 9, 1998). Oth-ers52have shown bed sharing with multiple familymembers in an adult bed to be particularly hazard-ous for the infant . Although overlying may be themechanism in some of these cases, soft sleep sur-faces, entrapment, and the likelihood of rolling to theprone position in such circumstances also may havea role.
9 The risk of SIDS associated with co-sleeping issignificantly greater among ,53 55 Some be-havioral studies have demonstrated that infants havemore arousals and less slow-wave sleep during bedsharing,56,57but no epidemiologic evidence exists thatbed sharing is protective against Birth and Low Birth WeightInfants born before term or who are low birthweight are at increased risk for SIDS, and risk in-creases with decreasing gestational age or ,5 The increased risk cannot be explained bya greater likelihood of apnea of prematurity amongpreterm SIDS victims while they are in the hospitalafter is unclear whether other complicationsof prematurity, such as bronchopulmonary dysplasiathat has been associated with SIDS, can explain asignificant amount of the increased risk associatedwith are no data suggesting thatstrategies designed to reduce risk in full-term infantsshould not also be applied to premature infants.
10 Therelationship to prone sleeping, for example, has beenshown to hold for infants of low birth weight as wellas for those born with a normal birth weight Thought to Protect Against SIDSA lthough several retrospective studies have dem-onstrated a protective effect of breastfeeding onSIDS,3,59other analyses and prospective cohort stud-ies failed to find such an effect after adjustment forconfounding 64 Although breastfeedingis beneficial and should be promoted for many rea-sons, the Task Force believes that evidence is insuf-ficient to recommend breastfeeding as a strategy toreduce recent studies have reported a substantiallylower SIDS incidence among infants who used pac-ifiers than among infants who do ,36,65,66Al-though this association has been strong and consis-tent, it does not prove that pacifier use preventsSIDS. Mechanisms by which pacifiers might protectagainst SIDS have been proposed, such as stinting ofthe upper airway, but data are lacking to demon-strate that any of them are relevant to SIDS.