Transcription of Assessment and Management of Chemical Coping …
1 Assessment and Management of Chemical Coping inPatients With CancerEgidio Del FabbroFrom Virginia Commonwealth Univer-sity, Massey Cancer Center, Richmond, online ahead of print on May 5, s disclosures of potential con-flicts of interest and author contribu-tions are found at the end of author: Egidio DelFabbro, MD, Palliative Care Program,Division of Hematology, Oncology andPalliative Care, Virginia CommonwealthUniversity, 1101 East Marshall St,Richmond, VA 23298-0230; 2014 by American Society of ClinicalOncology0732-183X/14/3216w-1734w /$ : Coping is a working definition that describes patients intake of opioids on a scale that spansthe range between normal nonaddictive opioid use for pain all the way to opioid addiction. Mostpatients will fall somewhere between the two extremes in using opioid analgesics to cope with theirpsychological or spiritual distress. The degree to which patients use their medications in a maladaptivemanner will determine their susceptibility to drug toxicity and harm.
2 When there are no obviouscancer-related causes for increased pain intensity, Chemical Coping and other patient-related factorssuch as delirium, somatization, and depression should be considered. As part of the initial evaluationof patients with cancer-related pain, a brief screening tool such as the CAGE questionnaire should beused to identify patients who may be at risk for Chemical Coping . Identifying patients at risk will allowclinicians to avoid unnecessary opioid toxicity, control pain, and improve quality of life. A structuredapproach for managing opioid use should be adopted, including standardized documentation, opioidtreatment agreements, urine drug screens, frequent visits, and restricted quantities of breakthroughopioids. All patients at risk should receive brief motivational interviewing with an objective, nonjudg-mental, and empathic style that includes personalized feedback, particularly about markers of risk orharm.
3 For Chemical copers approaching the addiction end of the spectrum, with evidence ofcompulsive use and destructive behavior, referral should be made to substance abuse Clin Oncol 32:1734-1738. 2014 by American Society of Clinical OncologyINTRODUCTIONMany patients treated for cancer have a high symp-tom burden, regardless of whether they are at theend of life or early in the cancer to severe levels of pain are reported in approxi-mately 15% of ambulatory patients with cancer andin 70% of those referred to palliative with these high-intensity pain levels re-quire a longer duration of therapy and higher opioiddoses to achieve pain control,3and almost half maynot respond at who report persistent,severe pain despite increasing doses of opioids are achallenge for the clinician, because cancer pain com-prises physical, psychological, social, and spiritualdimensions. Determining the contribution of eachdimension to the total pain experienced by the indi-vidual patient can be difficult.
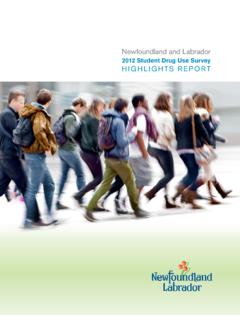
4 Cancer progression,new metastases, or complications such as pathologicfractures may account for increased pain in manypatients who seem not to respond to , when there are no obvious cancer-relatedcauses for the increased pain, clinicians should con-sider patient-related factors that may amplify painexpression, including delirium, somatization, de-pression, and Chemical Coping (Fig 1). Although apreliminary study showed that functional magneticresonance imaging4can discriminate between acutecutaneous pain and a form of social pain, there is noobjective measure for quantifying the chronic painexperienced by patients or determining the contri-bution of psychosocial factors that influence totalpain. Unfortunately, some patients reporting severepain may be requesting increasing doses of opioidsto cope with their psychological, spiritual, or exis-tential distress rather than their physical pain. Thesechemical copers are more likely to have a prior his-tory of alcoholism or substance abuse,5,6will typi-callyreceiveahighermorphineequivale ntdailydose(MEDD) for pain control, and are more likely toexperience opioid adverse at riskfor Chemical Coping should be screened and identi-fied so that strategies can be implemented to im-prove patient care and aid health care providersfacing the difficult dilemma of contributing to un-necessary opioid dose escalation and opioid adverseeffects or perhaps undertreating a patient requiringhigh-dose opioids for pain OF Chemical COPINGC hemical Coping is a working definition first used byBruera et al8that describes the intake by patientsJOURNAL OFCLINICALONCOLOGYREVIEW ARTICLEVOLUME 32 NUMBER 16 JUNE 1 20141734 2014 by American Society of Clinical OncologyDownloaded from by Francisco Pedrosa on July 29, 2014 from 2014 American Society of Clinical Oncology.
5 All rights cancer of opioids on a scale spanning the range between normalnonaddictive opioid use for pain all the way to total addiction and itsaccompanying compulsive, destructive behavior. Most patients willfall somewhere between the two extremes, using their medications innonprescribed ways to cope with their relationship be-tween addiction and Chemical Coping is summarized by Kirsh et al9asfollows: All addicts are Chemical copers but not all Chemical copersare addicts. 9(p221) Mild Chemical copers may not experience anymajor adverse effects, whereas those approaching the addiction end ofthe spectrum are at risk for increased morbidity and mortality. Thereis, therefore, a broad spectrum of Chemical Coping , and the degree towhich patients use their medications in a maladaptive manner willdetermine their susceptibility to drug toxicity and harm. Chemicalcoping and addiction should be distinguished from physical toleranceand withdrawal syndrome when opioids are abruptly is characterized by changes in brain structure and functionthat accompany chronic exposure to drugs of addiction was traditionally thought to be rare among patientstreated for , some of the same risk factors for addic-tion found in patients without cancer might also be found in thosewith cancer, such as alcohol and tobacco abuse, depression, general-ized anxiety disorder, post-traumatic stress disorder, psychologicaltrauma, illicit drug use, psychotropic medication use, antisocial per-sonality disorder, and childhood misconceptionabout the low risk for opioid misuse, coupled with an ongoing legiti-mate worry about the inadequate treatment of cancer-related pain.
6 13has regrettably diminished clinicians concern about substance abuseand Chemical Coping in patients with prevalence of Chemical Coping among patients with cancer isuncertain; however, there is evidence that a history of alcoholism, oneof the major risk factors for Chemical Coping , is common across thedisease trajectory. The prevalence of alcoholism has long been undera-ppreciated in general medical wards14and among oncology one third and 40% of male hospital patients are alcoholics15;however, a minority of these patients are identified, and an evensmaller group is referred for 705 male patients withupper digestive tract tumors assessed preoperatively, 81% were alco-hol misusers by Diagnostic and Statistical Manual of Mental DisordersIII criteria, although only 16% were detected by routine studies in patients with advanced cancer referred topalliative care have reported rates of alcoholism between 17%18and33%.
7 8 Although few studies have been conducted in hospice patients,more than one third of hospices in Virginia report that abuse anddiversion are problems in their OF Chemical COPINGS ubstance abuse can impede patients quality of life, increase thecomplexity of managing high physical and psychosocial needs, andlead to increased hospital admissions. As therapies for cancer treat-ment advance and patients survive for longer periods, the conse-quences of prolonged opioid use and high doses need tobe NeurotoxicityThe risks to patients include opioid-induced neurotoxicity, suchas excessive sedation, delirium,20myoclonus, and even seizures. Theserisks increase as a patient s Chemical Coping becomes increasinglymaladaptive and moves toward the addiction end of the doses of opioids are also associated with delirium in patientswith cancer, and as a result, opioids may contribute to intractabledelirium and a need for palliative patients receiving chronic opioids are tolerant to theeffects of respiratory depression, there is the potential for drugs, particularly opioids, are now the most commoncause of overdose, outstripping illicit drugs such as heroin and a study evaluating the characteristics of deaths result-ing from prescription drugs, a substance abuse indicator was presentin of the rate of overdose is lower amongpatients with cancer compared with other patients, a study from theVeterans Administration showed an increased overdose risk amongpatients with cancer receiving opioid therapy.
8 Especially if patientswere prescribed as-needed opioids alone compared with regularlyscheduled opioids Agents of Chemical CopingPatients identified as positive after screening for alcohol misusealso have a higher frequency of nicotine use. Continued smokingdespite a diagnosis of cancer should be considered maladaptive chem-ical Coping , because continued smoking increases the risk for cancerrecurrence, impairs treatment of the cancer, and impairs quality who are Coping chemically are also at increased risk forpolysubstance abuse with illicit drugs such as cocaine and heroin andare more likely to use benzodiazepines,26increasing the possibility ofexcessive sedation or accidental opioid-related ,28 SLIPPERY SLOPE: ANY BENEFIT OF Chemical Coping ?Although we are concerned primarily with unnecessary dose escala-tion and the adverse effects of potentially addictive prescribed drugs,preliminary studies do suggest that pharmacologic agents for painmightdecreasespiritual,psychological , bleedChemicalcopingDeliriumOpioid toleranceIncreasedPainPatient-Related FactorsCancer-Related FactorsDepressed mood or somatizationInfectionFractureFig and patient-related factors contributing to pain.
9 Data and Management of Chemical Coping in Patients With 2014 by American Society of Clinical Oncology1735 Downloaded from by Francisco Pedrosa on July 29, 2014 from 2014 American Society of Clinical Oncology. All rights means condones the use of opioids for purposes other than painrelief, such as psychological distress. Clearly, the suffering of patientswith cancer is compounded rather than diminished by substanceabuse. There should be recognition, however, that some of these painmedications may ameliorate psychological and social components oftotal pain. Recent advances in neuroscience show that there is overlapin the neurobiologic foundations of physical and social pain29and thatnegative affect, pain, and cognitive control are anatomically and func-tionally integrated in the cingulate evidence of themechanistic links between physical and social pain are provided bystudies showing that opioids may decrease separation distress,31andexperimentally, acetaminophen has been shown to decrease distress inhealthy people contemplating their own OF Chemical COPINGT here may be health care providers who are skeptical about the valueof identifying and managing patients with advanced cancer who are atrisk for misuse of opioids.
10 There may be an attitude that these patientshave a limited life expectancy, and there is no additional harm fromusing excessive amounts of , if we are to managesymptoms optimally and allow patients to fulfill their maximal phys-ical and psychosocial potential, we must avoid the adverse effects ofhigh-dose opioids and their detrimental effects on patients and fam-ilies quality of systematic review of chronic noncancer pain in patients whoalso have a substance use disorder concluded that little empiric dataare available to guide clinicians in treating these iseven less information regarding patients with cancer, and much of themanagement is driven by the universal precautions approach35,36toassessment and Management advocated for noncancer patients withchronic ,38An adaptation of this universal Management ap-proach is summarized in Table 1. Patients identified as at risk shouldenter an opioid agreement that outlines expectations, including re-ceiving prescriptions from a single provider.