Transcription of Bilevel Positive Airway Pressure Ventilation
1 Vol. 6, No. 9 JCOMO ctober 1999 41 OUTCOMES IN PRACTICEB ilevel Positive Airway Pressure VentilationSharon E. Mace, MD, FACEP, FAAPOver the past few decades, invasive Positive pressureventilation, usually applied via an endotrachealtube, has been the standard treatment for acute res-piratory failure [1 3]. However, intubation and mechanicalventilation is associated with significant morbidity, includ-ing upper Airway trauma and infections [4 7]; indeed, it isthe single most important predisposing factor for nosocomi-al pneumonia [7]. In response to the problems associatedwith intubation, noninvasive Positive Pressure Ventilation (NPPV) has become more common in the treatment of pa-tients with respiratory failure [7,8]. NPPV has the advan-tages of avoiding endotracheal tube related morbidity aswell as increasing patient comfort and autonomy; it also maybe more cost-effective [9 12]. Of the several types of noninvasive Ventilation , bilevelpositive Airway Pressure (BiPAP) has become the one mostcommonly used [13].
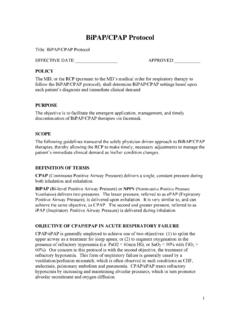
2 BiPAP ventilators (Figure) deliver apositive Airway Pressure that alternates between a higherpressure during inspiration and a lower Pressure duringexpiration. When the ventilator detects the patient s inspira-tion, it increases the inspiratory Positive Airway Pressure (IPAP) to a set level until it senses a drop in the flow ratebelow a given threshold value (usually 25% of the peakinspiratory flow) or until a certain amount of time elapses(usually 3 seconds). Then, the Pressure support ventilationdecreases to the expiratory Positive Airway Pressure (EPAP)level, which lasts until the patient s inspiration is againdetected and the cycle repeats. Because BiPAP is a relatively new ventilatory modality,many clinicians may be unfamiliar with its use. This articlereviews the utility of BiPAP in acute respiratory failure andprovides illustrative examples of its application in Positive Pressure mechanical Ventilation withuse of an invasive artificial Airway and NPPV work via simi-lar mechanisms.
3 Positive Pressure is transmitted through theupper Airway to the alveoli of the lungs, which increasestranspulmonary Pressure , inflates the lungs, and aids alveo-lar Ventilation [14] (Table 1).The inspiratory Positive Airway Pressure in BiPAP, func-tions to decrease the work of breathing. The expiratory posi-tive Airway Pressure in BiPAP acts to increase the functionalresidual capacity of the lung by recruiting collapsed functional residual capacity improves Ventilation -perfusion (V/Q) matching. At low lung volumes, small air-ways collapse so that the alveoli are perfused but not venti-lated; this can contribute to hypoxemia [7]. Like continuouspositive Airway Pressure (CPAP), BiPAP could cause anincrease in mean intrathoracic Pressure (which theoreticallycould decrease venous return to the heart and cardiac output)[15] and an increased or excessive alveolar Pressure distrib-uted to more compliant lung segments, which could lead tobarotrauma (eg, pneumothorax, pneumomediastinum) [16].
4 UsesBiPAP was initially used in the 1980s in patients with chron-ic respiratory failure such as those with obstructive sleepapnea, nocturnal respiratory muscle fatigue (associated withneuromuscular disorders such as muscular dystrophy, amy-otrophic lateral sclerosis, and multiple sclerosis), and thoracic cage deformities [17 20]. Its was then extended touse in patients with acute respiratory failure includingpatients with acute exacerbation of chronic obstructive pul-monary disease (COPD), asthma, congestive heart failure,and pulmonary edema [9,12,21,22] (Table 2). BiPAP repre-sents an advance over CPAP: although both BiPAP andCPAP provide a Positive end-expiratory Pressure , whichincreases functional residual capacity and decreases V/Qabnormalities, BiPAP helps decrease the patient s work ofbreathing by providing a higher level of Pressure supportduring inspiration. BiPAP can be used in pediatric as well asadult patients [23,24].
5 ComplicationsMost complications of BiPAP are minor (Table 3) and oftencan be avoided or minimized if adequate precautions aretaken. Minor injury to the skin of the face secondary to themask is probably the most common complication, occuringSharon E. Mace, MD, FACEP, FAAP, Associate Professor, Departmentof Emergency Medicine, Ohio State University School of Medicine,Director, Pediatric Education/Quality Improvement, Director, Obser-vation Unit, Cleveland Clinic Foundation, Cleveland, approximately 13% of patients [25 27]. Skin necrosis,ulcers, and lacerations can occur, especially if the mask fitspoorly. This side effect can be minimized by a properly fit-ting mask and occasionally by use of a patch or skin dress-ing applied to skin Pressure points (ie, the chin and bridge ofthe nose) [7]. In general, rapid spontaneous healing of theskin occurs in 2 to 7 days once mask use is discontinued [7].Irritation to the eyes from the mask Ventilation also canoccur.
6 Use of properly fitting equipment and a clear occlu-sive dressing will minimize this side effect. Irritation to thenasal mucosa or drying of the upper Airway passages can belessened or avoided by using distention is uncommon (incidence rate, 2%) [27].However, aspiration of gastric contents into the lung due toabdominal distention is a potential serious complication. Insome patients, insertion of a nasogastric tube may help avoidgastric distention. Avoidance of extremely high BiPAP pres-sures also should reduce the risk of this complication. It maybe prudent to avoid the use of BiPAP in patients with recentupper gastrointestinal surgery. Limiting oral intake decreas-es the possibility of gastric distention and possible aspira-tion. Patients on BiPAP generally take nothing by mouthexcept for small amounts of liquids and oral medications,although some clinicians allow patients on prolonged nasalBiPAP to take small meals. Ancillary staff (eg, nursing, respi-ratory therapy) should be instructed to observe the patientfor signs of abdominal hypoxemia secondary to accidental removal ofthe mask or disconnection of the BiPAP apparatus can monitoring of the patient by a dedicated nurseor respiratory therapist in the critical care setting (at least ini-tially), continuous pulse oximetry, and setting the BiPAPventilator alarms should help avoid this of BiPAP and/or worsening clinical condition canoccur.
7 Therefore, continuous patient monitoring, especiallyin the early stages of treatment in acute respiratory failurepatients, is mandatory. Although use of BiPAP can avoidintubation in 60% to 90% of patients [28], some patients willfail a trial of BiPAP and require intubation. Set-up prepara-tion and availability of equipment for achieving definitiveairway access is needed for all patients placed on for discontinuing BiPAP are shown in Table 4. ContraindicationsBiPAP is contraindicated in patients who are in cardiopul-monary arrest or who are hemodynamically or electrocar-diographically unstable [26]. Other contraindications are list-ed in Table has been raised regarding the possibility ofdecreased cardiac output with high levels of Positive airwaypressure [29 31]. However, this has generally been more of atheoretical concern. With CPAP, cardiac output decreasedslightly in some patients, but the decrease was not statistical-ly significant [15].
8 In patients with left ventricular dysfunc-tion, the cardiac output has actually increased [15,31 34].CPAP leads to a Positive intrathoracic Pressure . Thiscauses a decreased left ventricular transmural Pressure caus-ing a decreased left ventricular afterload. In patients with leftventricular dysfunction creating high filling pressures, thedecreased left ventricular afterload more than compensatesfor the decreased cardiac output caused by a decreasedvenous return. It is assumed that BiPAP will have similarhemodynamic effects to CPAP. However, this has yet to bewell increase in intracranial Pressure has been noted onlywith the use of CPAP in patients at risk for intracranial prob-lems such as in head-injured patients. BiPAP is probably notindicated in patients with increased intracranial pressure42 JCOMO ctober 1999 Vol. 6, No. ventilator (A) and patient on BiPAP using oronasal mask (B).ABbecause they would have other contraindications or limita-tions to the use of BiPAP such as apnea or an altered mentalstatus.
9 BiPAP is not contraindicated in other types of traumapatients [35].There is a time factor in the use of BiPAP. A finite periodof time is required to select and fit the mask and set up theapparatus, instruct the patient, and allow time for the patientto equilibrate at the chosen settings. Compared with con-ventional Ventilation , there may be a somewhat slower cor-rection of gas exchange abnormalities (eg, hypoxemia andhypercapnia). Thus, patients in extremis needing immediatecorrection of respiratory abnormalities are not candidates IssuesPatient SelectionThe patient should be alert, with an appropriate diagnosis(Table 2) and no contraindications. Patients must keep theirglottis open during Positive Pressure Ventilation to allow airto enter the alveoli. During nasal Ventilation , patients mustkeep their mouth closed or Airway Pressure will be must coordinate their respirations with the ventila-tor to allow the ventilator to assist their breathing.
10 For thesereasons, BIPAP can only be used in cooperative patients. Interface SelectionPatients on BiPAP usually wear a face mask (Figure) or anose mask. Although face-mask interfaces prevent air leak-age through the mouth, they interfere with speech and eat-ing, and a beard or moustache may make them difficult toadjust. In practice, face masks are often used in acute settingssuch as the emergency department. Ventilator SettingsThe physician chooses the parameters for the initial ventila-tor settings: IPAP, EPAP, I:E ratio, mode, and, on newer mod-els, the fraction of inspired oxygen (FIO2). The usual range forIPAP is 10 to 20 cm H2O and the usual range for EPAP is 5 to10 cm H2O. IPAP must be greater than EPAP. The I:E is theratio of inspiratory time to expiratory time and is usually setat 1:3 or 1:4, which allows sufficient time for expiration andVol. 6, No. 9 JCOMO ctober 1999 43 OUTCOMES IN PRACTICET able of BiPAP on Respiratory PhysiologyOverall effectsDecreases total lung resistanceIncreases lung complianceDecreases work of breathing by decreasing the energy neededto reinflate the alveolar sacs with each inspirationIncreases end-expiratory lung volumePrevents expiratory alveolar collapseAlveolar patency throughout both phases of respiratory cycleallows more time for gas exchange (causing increased arterialoxygenation and CO2elimination)May overcome the closing Pressure of a surrounding obstruction(eg, tumor)Increases functional residual capacityIncreases surface area of alveoli (increased gas exchange anddecreased V/Q shunting)Recruits more alveoli (fewer closed alveoli)Possible decrease in left ventricular afterload due to increasein intrathoracic Pressure and possible increase in preloadSpecific effectsIPAP Decreases work of breathingImproves minute Ventilation (VE)Decreases elevated CO2(treats hypercarbia)