Transcription of Claims submission made easy - Aetna International
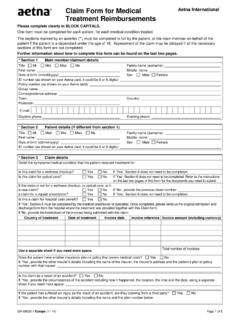
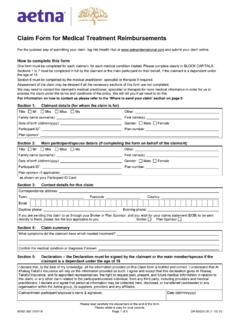
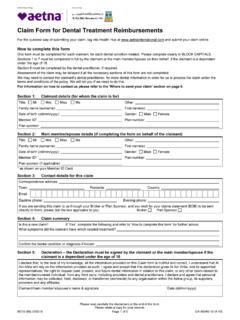
1 Questions? We know you may have questions and we're always here to help. You can call us any time on the phone number listed on the back of your Aetna ID Card. You can also send us a secure email by logging in to and clicking 'Contact us'. Claims submission made easy Some services may require This form can be used to submit a additional information claim for medical, dental, vision, or For some services, you'll need to submit additional documents. If your claim falls into any of the pharmaceutical services. categories below, you'll need to provide the additional items listed. If you're filing a claim for more than one person, a Prosthetic services (such as crowns, bridges or separate form is needed for each family member. dentures): X-rays (or the dentist's narrative report, if x-rays are not How to Fill in this Form available).
2 Complete the entire form using black ink A dental chart showing any missing teeth and dates of Mark your answers, where applicable, with an 'X', like this: [ extraction Date of prior prosthetic placement with a rationale for Double check to make sure your payment details are accurate replacement if applicable Sign and date the authorization Write your member identification number on each document Periodontal services: submitted with your claim form X-rays Keep a copy of your completed form for your records Current dated pre-operative periodontal charting Submitting your claim Once you have completed the claim form, you'll need to submit it along with your itemized bills and receipts. If your receipts are small, you Orthodontic services: should tape them on to a full size piece of paper. Then, submit the Date appliance was placed documents whichever way you prefer.]
3 We will process your claim and Number of months of treatment respond within 10 to 14 calendar days. Number of months of treatment remaining Upload it*. Log in at and click ' Claims Center' Services relating to accidental injury Fax it Pre-treatment X-rays Outside the US: +1 800 475 8751 (via AT&T + access code) Details of the accident Inside the US:+1 859 425 3363. Email it*. If your plan requires school attendance as a Send attachments to condition of coverage for dependents over a Mail it certain age, you may need to provide: Aetna International / Aetna . PO Box 981543, El Paso, TX 79998-1543, USA. a report card, tuition statement or other form of school For Claim Status or Service, Call: attendance verification Outside the US: +1 800 231 7729 (via AT&T + access code). Collect outside the US or Direct:+1 813 775 0190.
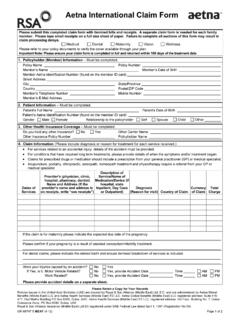
4 * Attachment limit size is 10MB. GR-68069 (9-16) E R-POD. Subscriber's Name (First Name, Middle Initial, Last Name/Surname) Page 1. 1 Personal details About the member (subscriber) About the employer Name (as shown on your Aetna ID card including full First name) Name First name(s): Last name/Surname: Group number Aetna ID number (as shown on your Aetna ID card). Date of birth Gender About the patient Name M M D D Y Y Y Y Male Female First name(s): Contact details Last name/Surname: Telephone number (include Area &/or Country Code): Date of birth Gender Email address: M M D D Y Y Y Y Male Female Address Relationship to member Street Address: Self Spouse Child Other: City: State/province: Country: Postal/ZIP code: 2 Reimbursement details Out-of Network Providers Outside the The manner of reimbursement may consist of payment in (i) the Where would you like reimbursement to be sent?
5 Applicable local currency subject to the principle of indemnity we mention above (if feasible at the sole discretion of Aetna ), or (ii) if you do To the member (subscriber) To the provider not have a bank account in such local currency, in the currency in which What payment details should we use to reimburse you? the policy premium was paid in an amount equal to the applicable Use the Recurring Reimbursement Election (RRE) Reasonable and Customary Charges. information currently on file Use the information provided in the Payment Details section Payment details below to establish an RRE, or update your current RRE If you have chosen to receive your benefits by bank transfer, please complete the details below. Use the information provided in the Payment Details section below only for expenses related to this form We will transfer funds to your bank at no cost to you, but we encourage you to please check with your bank to determine whether your bank How should we process your reimbursement?
6 May charge you any additional fees for receiving Funds Transfers. By bank funds transfer from Aetna to the bank account given below. This is the easiest way of reimbursement. Name of Bank Accountholder (as it appears on Bank Statement). By check What currency would you like to be reimbursed with, GBP? Bank Account number If the currency chosen is not available for the reimbursement method selected above, we will default to a US Dollar ($) wire, if bank details are available, or a US Dollar ($) check payable to Bank Identification Code/Routing number or Alternative ID / Code the party to which payment is sent, if no bank details exist. Country: Code (wire only) CHIPS UID Federal ABA. Currency: Bank Sort ID IBAN* Other**. Reimbursement for Providers Outside of the (* Please check with your bank to confirm any IBAN requirements, which, in If, acting reasonably, we determine that any central bank or relevant certain countries, are mandatory and must be supplied for bank funds transfer government or governmental authority imposes an artificial exchange rate claim payment transactions, such as in the United Arab Emirates (UAE).)
7 (including without limitation an exchange rate which is inconsistent with the free ** Use Other entry field to describe reported Alternative IDs or Codes such as market exchange rate) in relation to a relevant currency for any reason, we may Bank Code/Branch, RUT#, IFSC Code, KBA#. in our sole discretion reimburse you for your valid Claims pursuant to this agreement for treatment in such country in any manner we may reasonably Bank details decide. In making such determination we shall seek to ensure that, in keeping with the fundamental basis of any contract of insurance, we indemnify you for Bank name: your loss (subject to the terms and conditions of your policy) but do not unjustly Street address: enrich you as may have been the case had we applied such artificial exchange rate to pay you in another currency. City: Aetna In-Network Providers Outside the The manner of reimbursement may consist of payment in (i) the applicable local State/province: currency (if feasible at the sole discretion of Aetna ), or (ii) if you do not have a Country: bank account in such local currency, in the currency in which the policy premium was paid in an amount equal to that which we would have paid our network Postal/ZIP code: provider in the currency in which premium was paid pursuant to our obligations Telephone number (include Area &/or Country Code): to such network provider (as we may reasonably determine), subject in each case to the principle of indemnity we mention above.
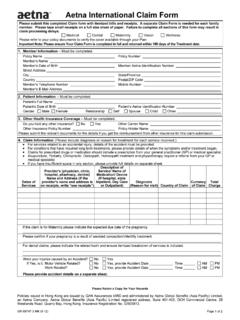
8 GR-68069 (9-16) E Please Retain A Copy For Your Records Subscriber's Name (First Name, Middle Initial, Last Name/Surname) Page 2. 3 Claim details What type of service(s) are you filing a claim for? Refer to your plan documents to verify the coverage(s) that are available through your Plan. Medical Pharmacy Dental - please attach form GC-14423 Vision (Identify the related tooth number for all dental procedures). Respond Yes or No . The claim is related to a work related accident or condition. Yes No The claim is related to an accidental injury. Yes No If you're submitting a claim for a work-related accident or condition, or an accidental injury, please give the details: Date of accident Time M M D D Y Y Y Y H H M M AM PM. How and where did the accident occur? Please note: Use the space below to summarize each instance of treatment you're filing a claim for.
9 If you need to submit a claim for more than two instances, please also complete Page 3 and return it along with this form. Check here if only the Treatment Summaries below are included for this claim submission . Treatment summary Treatment summary Treatment date Total charge (with currency) Treatment date Total charge (with currency). M M D D Y Y Y Y M M D D Y Y Y Y. Location of claim Provider's name and address Location of claim Provider's name and address City: City: State/province: State/province: Country: Country: Postal/ZIP code: Postal/ZIP code: Description of service Description of service type of treatment, name of medication/device type of treatment, name of medication/device Reason for visit Reason for visit Type of patient Type of patient Inpatient Outpatient Inpatient Outpatient If in If in What was the admit date?
10 And the discharge date? What was the admit date? And the discharge date? M M D D Y Y Y Y M M D D Y Y Y Y M M D D Y Y Y Y M M D D Y Y Y Y. GR-68069 (9-16) E Please Retain A Copy For Your Records Subscriber's Name (First Name, Middle Initial, Last Name/Surname) Page 3. Please note: Use the space below to summarize each instance of treatment you're filing a claim for. If you need to submit a claim for more than the two additional instances (below), please copy this page before you go any further and return any additional sheets along with this form. Please renumber the Page Numbers of the additional copies beginning with Page 5. Treatment summary Treatment summary Treatment date Total charge (with currency) Treatment date Total charge (with currency). M M D D Y Y Y Y M M D D Y Y Y Y. Location of claim Provider's name and address Location of claim Provider's name and address City: City: State/province: State/province: Country: Country: Postal/ZIP code: Postal/ZIP code: Description of service Description of service type of treatment, name of medication/device type of treatment, name of medication/device Reason for visit Reason for visit Type of patient Type of patient Inpatient Outpatient Inpatient Outpatient If in If in What was the admit date?