Example: bankruptcy
COVID-19 Vaccination Clinic Demographic Form
COVID-19 Vaccination Clinic Demographic Form Name (as it appears on piece of identification) ... Out of Province Health Card ... Physician or Nurse Practitioner) Name . Author: Gina Bhullar
Tags:
Information
Domain:
Source:
Link to this page:
Documents from same domain

APPENDIX A Sample COVID-19 Vaccination Policy
www.healthunit.comAPPENDIX A – Sample COVID-19 Vaccination Policy [POLICY TITLE] (e.g., COVID-19 VACCINATION POLICY) PURPOSE To ensure that [Organization’s Name] employees are adequately immunized to minimize their risk of infection and to reduce the risk of transmission to others. POLICY STATEMENT

APPENDIX C Sample COVID-19 Vaccination Medical …
www.healthunit.comAPPENDIX C – Sample COVID-19 Vaccination Medical Exemption Form MEDICAL EXEMPTION TO DECLINE THE COVID-19 VACCINE _____ has a medical exemption for the COVID-19 Vaccine in Printed Name of Employee relation to a condition indicated below. The following conditions are the only absolute medical exemptions from the COVID-19 vaccine: ...

6. Infection Control Policy (Sample) Infection Control
www.healthunit.comand use routine infection control precautions and; 2) are aware of recommended immunizations for adults that help to prevent the transmission of infections amongst employees. POLICY: All staff will adhere to routine infection control precautions and will keep immunization status up to date in accordance with Ministry of Health

HEALTH CARE PROVIDER INFLUENZA VACCINE CONSENT …
www.healthunit.comI consent to receiving the seasonal influenza vaccine. If signing for someone other than yourself, indicate your relationship to that other person: _____ If signing for someone other than myself, I confirm that I am the parent / legal guardian or substitute decision maker.

14. No Smoking Policy (Sample) POLICY
www.healthunit.comSmoking is prohibited at all times, with the exception of during specified breaks, at which time the employee must smoke in designated outdoor areas. 4. No Smoking signs must be posted at all entrances and exits, washrooms, and in workplace vehicles. 5. If an employee does not comply with this policy, the issue will be dealt
Related documents

Medical Assistant Registered Application Packet
www.doh.wa.govmedical assistant-registered by the same Healthcare practitioner, clinic, or group practice and you renew your registration. • Your registration based on an endorsement by a healthcare practitioner, clinic, or group practice is not transferable to another healthcare practitioner, clinic, or group practice.

solated Patients ravel and Accommodation Assistance ceme …
www.iptaas.health.nsw.gov.au13. Referring practitioner details Full name Phone number ( ) 14.reatment details T Name of practitioner or health service you referred the patient to Treatment location Type of treatment referred for Is the practitioner or health service the nearest to the patient’s residence? Yes Go to question 15 oN Give details below

An Explanation of Standardized Procedure Requirements for ...
rn.ca.govpractitioner. Organized health care systems includes health facilities, acute care clinics, home health agencies, physician’s offices and public or community health services. Standardized procedures means policies and protocols formulated by organized health care systems for the performance of standardized procedure functions.

General Information: Nurse Practitioner Practice
www.rn.ca.govGENERAL INFORMATION: NURSE PRACTITIONER PRACTICE Scope of Practice. The nurse practitioner (NP) is a registered nurse who possesses additional preparation and skills in physical diagnosis, psycho-social assessment, and management of health- illness needs in primary health care, who has been prepared in a program that conforms to Board
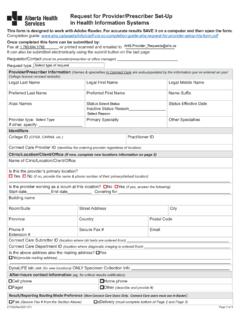
Request for Provider/Prescriber Set-Up in Health ...
www.albertahealthservices.caRequest for Provider/Prescriber Set-Up in Health Information Systems (Rev-) Page 3 of 3 eDelivery Data Source Grid Select this box to set up provider(s) to receive the same data types as other provider(s) at the same clinic (Skip Part A & B) All eDelivery recipients will be set up to receive Connect Care Results, including: Lab, DI, Cardiology, Endoscopy, and Documentation.

Immunization Form Name - Minnesota Department of …
www.health.state.mn.us• Your doctor or clinic can provide a copy of your child’s immunization history. If you are missing or need information about your child’s immunization history, talk to your doctor or call the Minnesota Immunization Information Connection (MIIC) at 651-201-3980 or 800-657-3970. 2. Sign or get the signatures needed for the back of this form.

Page 1 Day 1 Starting Suboxone (buprenorphine/naloxone)
www2.gov.bc.caContact Information Patient Name Provider Name Provider Number Most people feel much better by the end of the first day. Contact your provider if you are still feeling bad withdrawal or feel like using and have taken the daily max of 12 mg. Day 1 Starting Suboxone® (buprenorphine/naloxone) Page 1

Regulations and Documentation Templates Guidance
www.omh.ny.govNurse Practitioner (NPP). This service may be provided to the client and/or collateral. Sessions less than 45 minutes will not be reimbursed by Medicaid. Rounding is not permitted. 45 minutes • Evaluation and Management (E & M) • Comprehensive Assessment • Health Screen Others noted above, as Needed