Transcription of CPD PAPER Endodontics: Part 1 The modern …
1 PRACTICEBRITISH DENTAL JOURNAL VOLUME 197 NO. 4 AUGUST 28 2004181 endodontics : part 1 The modern concept of root canal treatmentP. Carrotte1 root canal treatment has changed considerably since the hollow tube theory was first postulated in 1930. Research continuesinto the elaborate anatomy of root canal systems, and also into the microbial causes of endodontically related diseases. Only byunderstanding these aspects in detail can the practitioner quickly and effectively shapethe main root canals to facilitatethorough cleaningof the entire system, and easy and effective filling. root canal treatment is normally prescribed to treat an infection, and as with all surgicalprocedures an aseptic technique is essential throughout. As research has shown that success is only achieved when all microorganisms are removedfrom the entire root canal system, the anatomy of this system must be understood for eachtooth.
2 modern endodontic practice is concerned not with the old clich of cleaning, shapingandfilling, but with shapingfirst, to open the canals wide, so that cleaningcan be effectivelycarried out prior to three-dimensional BRIEFIn 1965 Kakehashi, Stanley and Fitzgerald1showed conclusively that pulpal and endodonticproblems are primarily related to microbial con-tamination of the root canal system. Since thattime endodontology has increasingly focussedon the ways and means of eliminating micro-organisms from the entire root canal system. The majority of patients who require rootcanal treatment will have been diagnosed as suf-fering from the disease of periradicular peri-odontitis. The treatment of this disease mustaddress the microbial contamination of theentire root canal system. It must also be carriedout under aseptic conditions in order to preventfurther microbial ingress, in particular from use of a rubber dam very much reflects theuse of a surgical drape in other invasive medicalprocedures.
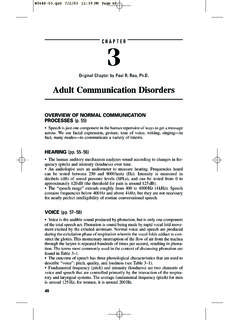
3 Such a biological approach will beemphasized throughout this text. The temptationto regard root canal treatment as a purelymechanical procedure, producing excellentpost-operative radiographs but with little regardto diagnosis and prognosis, must be resisted intoday s into the morphology of the pulp hasshown the wide variety of shapes, and the occur-rence of two or even three canals in a is a high incidence of fins which runlongitudinally within the wall of the canal and anetwork of communications between canalslying within the same root (Fig. 1). The manynooks and crannies within the root canal systemmake it impossible for any known technique,either chemical or mechanical, to render it total-ly sterile. The objective of treatment must be toreduce the level of microbial contamination asfar as is practical, and to entomb any remainingmicroorganisms with an effective three-dimen-sional prime aim when preparing the root canalhas long been stated as cleaning and of the prime aims of this text will be toencourage the practitioner to see this inreverse, ie shaping and cleaning.
4 Moderninstruments and techniques will be describedwhich rapidly open and shape the main root1 ENDODONTICS1. The modern concept ofroot canal treatment2. Diagnosis and treatmentplanning3. treatment of endodonticemergencies4. Morphology of the rootcanal system5. Basic instruments andmaterials for root canaltreatment6. Rubber dam and accesscavities7. Preparing the root canal8. Filling the root canal system9. Calcium hydroxide, rootresorption, endo-periolesions10. Endodontic treatment forchildren11. Surgical endodontics12. Endodontic problemsFig. 1 The rootcanal system ofthis lower molarhas been stainedand the toothtotally decalcified,showing thecomplex nature ofthe root canalsystem. (Courtesyof Professor R TWalker.)1*Clinical Lecturer, Department of AdultDental Care, Glasgow Dental Hospital andSchool, 378 Sauchiehall Street, Glasgow G2 3JZ*Correspondence to: Peter CarrotteEmail: British Dental Journal 2004; 197:181 183 VERIFIABLE CPD PAPERNOW AVAILABLE AS A 26/07/2004 15:09 Page 181 PRACTICE182 BRITISH DENTAL JOURNAL VOLUME 197 NO.
5 4 AUGUST 28 2004canals, thus permitting the effective access ofantimicrobial irrigants to the entire root canalsystem, including lateral canals, fins, anasta-moses and other canal aberrations. It is imper-ative that these instruments are not seen asproviding a route to quick and speedy rootcanal treatment . To achieve success the timesaved by the rapid opening of the canal systemmust be spent in thorough and effectiveantimicrobial has also shown that when an infect-ed root canal is accessed, the number of differentspecies of microorganisms is small, rarely abovesingle will become far moredifficult and extended, and success may well becompromised, if this flora is altered by theingress of saliva. Isolation of the tooth undertreatment is essential not only for medicolegalreasons to protect the airway, but, far moreimportantly, to prevent further contamination ofthe root canal system and to permit the use ofstrong intracanal areas of research have had the signifi-cant effect of changing the approach toendodontic treatment .
6 The hollow tube theoryput forward by Rickert and Dixon in 19314postulated that tissue fluids entering the rootcanal stagnated and formed toxic breakdownproducts which then passed out into the peri-apical tissues. This theory, that dead spaceswithin the body must be obturated, originallyformed the basis for filling root canals. How-ever, a variety of different studies havedemonstrated that, on the contrary, hollowtubes are tolerated by the body. As a resultthere are currently two indications for filling aroot canal , once the canal system has beenshaped and cleaned. Firstly, to prevent theentry of microorganisms to the root canal sys-tem from either the oral cavity, should thecoronal restoration leak or fail, or via thebloodstream (anachoresis). Secondly, to pre-vent the ingress of tissue fluid which wouldprovide a culture medium for any bacteriaremaining within the tooth following report by Klevant and Eggink5is particular-ly relevant.
7 They shaped and cleaned a numberof root canals, but the experimental group werenot obturated. They ensured that an effective,well-sealed, coronal restoration was found that healing occurred in every 2 shows a lower molar with a large peri-radicular lesion. The root canal system wasshaped and cleaned, and an intervisit dressing ofcalcium hydroxide placed. The patient did notreturn for further treatment for 6 months, when aradiograph revealed that complete healing hadtaken place. Of course, this does not mean that obturation isunimportant. It is essential for the reasonsdescribed earlier. It does prove, however, the oldclich that it is what is removed from the canalthat is important, not what is put in. Similarly,Ray and Trope6found that root -treated teeth witha poor obturation on radiograph but a good coro-nal restoration had a better prognosis than teethwith a good obturation but a poor majority of root canal sealers are solubleand their only function is to fill the minutespaces between the wall of the root canal and theroot filling material.
8 Their importance, judgedby the number of products advertised in the den-tal press, has been over-emphasized. Despitemuch research, gutta-percha remains the rootfilling of choice, although it is recognized that abiologically inert, insoluble and injectable pastemay be better suited for obturation of the rootcanal. Most of the new root canal filling tech-niques are concerned with methods of heatinggutta-percha, making it softer and easier toadapt to the irregular shape of the canal wall. Itmust be emphasized, however, that, whateverthe obturation system used, if the root canal sys-tem has not been adequately cleaned healingmay not occur (Fig. 3).Finally, lesions of endodontic origin whichappear radiographically as areas of radiolucencyaround the apices or lateral aspects of the rootsof teeth are, in the majority of cases, ,8 The lesions are the result of toxins produced bymicroorganisms lying within the root canal sys-tem.
9 This finding suggests that the removal ofmicroorganisms from the root canal followed byroot filling is the first treatment of choice, andFig. 2 (a) The pre-operative radiograph of tooth LR6 (46) shows a largeradiolucent area associated with the root apex and the furcation area. Rootcanal treatment was commenced. (b) A radiograph 6 months later whenthe patient finally returned to continue treatment shows evidence of bonyrepair with a return to a normal periodontal ligament space around theapex and in the 26/07/2004 15:11 Page 182 PRACTICEBRITISH DENTAL JOURNAL VOLUME 197 NO. 4 AUGUST 28 2004183that periradicular surgery, including an apicec-tomy with a retrograde filling, can only be sec-ond with a retrograde fillingat the apex is carried out in the hope of merelyincarcerating microorganisms within the tooth,but does not take into account the fact thatapproximately 50% of teeth have at least onelateral canal .
10 The long-term success rate ofapicectomy must inevitably be lower thanorthograde root summary, the principles of treatment of thedisease of periapical periodontitis are as : Produce a gradual smooth taper in theroot canal with its widest part coronallyand the narrowest part at the apicalconstriction, which, as discussed in part 4, is normally about 1 mm short ofthe : Use antimicrobial agents to removemicroorganisms and pulpal debris fromthe entire root canal : Obturate the canal system with an inert,insoluble filling material. 1. Kakehashi S, Stanley H R, Fitzgerald R. The effects ofsurgical exposures of dental pulps in germfree andconventional laboratory rats. J South California DentAssoc 1966; 334: 449 Burns R C, Herbranson E J. Tooth Morphology andCavity Preparation, Chapter 7 in Cohen S and BurnsR C, Pathways of the Pulp,St Louis 2002: Molven S, Olsen I, Kerekes K.