Transcription of CRISIS PLANNING TOOLS FOR FAMILIES
1 CRISIS PLANNING TOOLS FOR FAMILIES : A Companion Guide for Providers FINAL VERSION: March 29, 2011 1 CONTENTS INTRODUCTION BY PPAL .. 1 1: FAMILY-CENTERED SAFETY PLANNING .. 2 2: OVERVIEW OF CRISIS PLANNING TOOLS .. 4 COMPONENT I: SAFETY PLAN .. 4 COMPONENT II: ADVANCE COMMUNICATION TO TREATMENT PROVIDER (ADVANCE COMMUNICATION) .. 4 COMPONENT III: SUPPLEMENTS TO THE ADVANCE COMMUNICATION OR SAFETY PLAN .. 5 3: TIPS TO GUIDE PERSONS/ FAMILIES IN THE DEVELOPMENT OF A SAFETY PLAN .. 7 PROVIDER/ team CONSIDERATIONS .. 7 SETTING THE STAGE FOR SAFETY PLANNING .. 10 COMPLETION OF THE SAFETY PLAN TEMPLATE.
2 12 TESTING "USABILITY" .. 15 ADVANCE COMMUNICATION TO TREATMENT PROVIDER (ADVANCE COMMUNICATION) TEMPLATE .. 16 SUPPLEMENTS TO THE ADVANCE COMMUNICATION OR SAFETY PLAN20 INDIVIDUALIZED ALTERNATIVES .. 21 ROUTING BOXES .. 22 4: SAMPLE PLANS .. 23 SAMPLES OF TEMPLATE DOCUMENTS .. 25 5: RESOURCE 32 1 INTRODUCTION BY PPAL The Parent/Professional Advocacy League (PPAL) would like to thank all the FAMILIES who provided feedback for the revision and development of these new CRISIS PLANNING TOOLS . We would also like to thank the Massachusetts Behavioral Health Partnership (MBHP) for soliciting and incorporating the feedback of FAMILIES into these TOOLS .
3 PPAL is pleased that the voices and concerns of FAMILIES have been heard and heeded in making sure that both the CRISIS PLANNING TOOLS and CRISIS interventions are family-centered, youth-driven and culturally competent. Since 1996, when PPAL first published the CRISIS PLANNING Guide for FAMILIES with children who have mental health needs, we have worked to help FAMILIES design and decide upon plans that make sense for them and their children. The first handbook provided clear information and organized exercises for FAMILIES to prepare in advance of mental health crises with their children. Then in 2001, PPAL published the Police Pocket Guide, written by two mothers and informed by the personal experiences, both positive and negative, of thousands of FAMILIES with law enforcement officers.
4 The premise of this guide is that a sensitive and thoughtful interaction with a youth and their family leads to a more positive outcome than standard operating procedures. Twenty years of working with FAMILIES have demonstrated that there are no standard operating procedures that fit for all FAMILIES . FAMILIES deserve interventions that are tailored to their unique needs, based on their strengths and considerate of their own culture. More importantly, it is only when FAMILIES are truly the center of all during times of hope can be inspired and progress can be achieved. These newly revised CRISIS PLANNING TOOLS are a further example of how the desires and concerns of FAMILIES have been used as the basis of CRISIS PLANNING , and their voices have been validated.
5 2 1: FAMILY-CENTERED SAFETY PLANNING The safety PLANNING process and any resulting Safety Plan must be useful to the full array of children, FAMILIES , and young adults who receive Children s Behavioral Health Initiative (CBHI) services in Massachusetts. This includes parents with a pre-school age child in CRISIS as well as parents whose young adult child is in CRISIS . It includes persons/ FAMILIES that are wary of formal treatment services or have had negative experiences. It includes young adults who are seen involuntarily in an emergency room. It includes persons/ FAMILIES experiencing their first CRISIS episode, parents seeking help for children who don t want assistance, and children seeking help who do not feel supported by their parents.
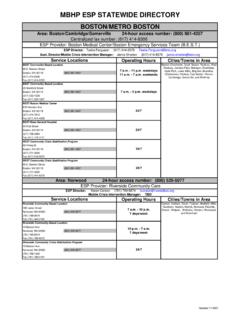
6 It includes persons/ FAMILIES from a range of cultures and beliefs who bring with them past experiences and personal biases; persons/ FAMILIES who are public about their struggles as well as persons/ FAMILIES who are private about them; and persons/ FAMILIES who have accepted and understand what is happening as well as persons/ FAMILIES who have not and do not. As many as 40 percent of persons seen by Emergency Service Program (ESP) teams in Massachusetts have not been previously seen by the CRISIS team and are not receiving other behavioral health services. A first experience in receiving CRISIS services can be daunting.
7 Engaging persons/ FAMILIES in the process, creating a comfortable environment, and achieving a consensus plan for what should happen next is essential not just for reducing risk in the current CRISIS episode, but in any future CRISIS episodes. Our greatest goal in safety PLANNING is that the process and any resulting products or plans will help to reduce unsafe situations and the likelihood of harm. In order for this goal to be realized, the person/family must actually use the plan in the event of a CRISIS . A plan may look terrific on paper, but if a family does not use it, what good has it served? If a comprehensive plan is developed for a family who is only ready for and interested in a pragmatic "If this, then this" type of plan, the efforts have been useless.
8 An unauthentic plan that is largely developed for rather than with a person/family can actually increase risk. As with all treatment services, it is important to consider timing, readiness, value as perceived by the recipient, and personal/familial priorities. An unwanted/un-useful process or off-putting product is not person/family-centered. The process/product may be perceived as an indication that the provider wasn't listening, isn't helpful, and doesn't care. The person/family may not seek the same services willingly in the future. If a person/family does not trust the system or becomes reluctant or unwilling to seek CRISIS services, risk increases.
9 If a person/family calls for CRISIS support or intervention, and the team or provider relies on a Safety Plan that lacks authenticity, then the team or provider runs the risk of misunderstanding the person/family and what they are willing/able to do and of misunderstanding the nature of the real risk. EXAMPLE: If the Safety Plan indicates that 14 year old Johnny will "punch his pillow, shoot baskets or draw in a notebook when he is starting to feel angry and get aggressive," then the team providing CRISIS support or intervention might assume that Johnny has insight into the 3 nature of his behavior, has developed useful coping strategies, AND believes those strategies could work.
10 If in reality Johnny has little insight into the nature of his anger, rarely "feels it coming on," hasn't developed effective strategies, and didn't participate in a meaningful way in CRISIS PLANNING then the Safety Plan lacks authenticity, and a key risk factor of "poor insight" is not apparent. In person/family-centered service provision, creating a Safety Plan involves the provider joining with the person/family as they develop a plan that is truly representative of them. The provider is not the "leader," "expert," or "the one who knows best" about how to manage risk in this family. Rather, the provider's role here is to facilitate, guide, and empower the person/family in the creation of a Safety Plan that reflects not what the provider necessarily wants the person/family to do but rather what the person/family will actually do in the event of a CRISIS .