Transcription of Diagnosis and management of hemochromatosis: 2011 …
1 AASLD PRACTICE GUIDELINED iagnosis and management of hemochromatosis :2011 Practice Guideline by the american Associationfor the Study of Liver DiseasesBruce R. Bacon,1 Paul C. Adams,2 Kris V. Kowdley,3 Lawrie W. Powell,4and Anthony S. Tavill5 This guideline has been approved by the AmericanAssociation for the Study of Liver Diseases (AASLD)and represents the position of the recommendations provide a data-supportedapproach to establishing guidelines. They are based onthe following: (1) a formal review and analysis of therecently published world literature on the topic; (2)the american College of PhysiciansManual for Assess-ing Health Practices and Designing Practice Guidelines1;(3) guideline policies including the AASLD Policy ontheDevelopment and Use of Practice Guidelinesand theAmerican Gastroenterological association sPolicy State-ment on the Use of Medical Practice Guidelines2; and(4) the experience of the authors in regard more fully characterize the available evidencesupporting the recommendations, the AASLD PracticeGuidelines Committee has adopted the classificationused by the Grading of Recommendation Assessment,Development, and Evaluation (GRADE) workgroupwith minor modifications (Table 1).
2 3 The strength ofrecommendations in the GRADE system are classifiedas strong (class 1) or weak (class 2). The quality ofevidence supporting strong or weak recommendationsis designated by one of three levels: high (level A),moderate (level B), or low-quality (level C).Intended for use by physicians, these recommenda-tions suggest preferred approaches to the diagnostic,therapeutic, and preventive aspects of care. They areintended to be flexible in contrast to standards of care,which are inflexible policies to be followed in everycase. Specific recommendations are based on relevantpublished ,4 IntroductionHereditary hemochromatosis (HH) remains themost common, identified, genetic disorder in Cauca-sians. Although its geographic distribution is world-wide, it is seen most commonly in populations ofnorthern European origin, particularly Nordic orCeltic ancestry, in which it occurs with a prevalence ofapproximately 1 per 220-250 ,6 Thepathophysiologic predisposition to increased, inappro-priate absorption of dietary iron may lead to the devel-opment of life-threatening complications of cirrhosis,hepatocellular carcinoma (HCC), diabetes, and heartAll AASLD Practice Guidelines are updated annually.
3 If you are viewing a Practice Guideline that is more than 12 months old, please visit foran update in the : AASLD, american association for the Study of Liver Diseases; ALD, alcoholic liver disease; ALT, alanine aminotransferase; AST, aspartateaminotransferase; BMP6, bone morphogenetic protein-6; C282Y, Cys282 Tyr mutation; GRADE, Grading of Recommendation Assessment, Development, andEvaluation; H63D, His63 Asp mutation; HAMP, hepcidin; HCC, hepatocellular carcinoma; HH, hereditary hemochromatosis ; HIC, hepatic iron concentration;HII, hepatic iron index; HJV, hemojuvelin; OLT, orthotopic liver transplantation; PCT, porphyria cutanea tarda; S65C, Ser65 Cys mutation; TfR2, transferrinreceptor-2; TS, transferrin the1 Division of Gastroenterology and Hepatology, Saint Louis University School of Medicine, Saint Louis, MO;2 Department of Medicine, University ofWestern Ontario, London Health Sciences Centre, London, Ontario, Canada;3 Center for Liver Disease, Virginia Mason Medical Center, Seattle, WA;4 Royal BrisbaneHospital, University of Queensland Centre for Clinical Research, Brisbane, Australia; and5 Department of Gastroenterology, Case Western Reserve University, andDepartment of Gastroenterology and Hepatology, The Cleveland Clinic, Cleveland, March 22, 2011; accepted March 23, reprint requests to: Bruce R.
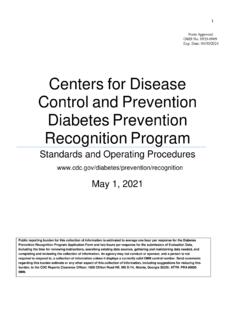
4 Bacon, , James F. King, , Endowed Chair in Gastroenterology, Professor of Internal Medicine, Divisionof Gastroenterology and Hepatology, Saint Louis University School of Medicine, Saint Louis University Liver Center, 3635 Vista Avenue at Grand Boulevard,St. Louis, MO 63110-0250. E-mail: fax: by the american association for the Study of Liver this article online at conflict of interest: Nothing to The principalHFEgene defect was firstdescribed in 1996, and is a G-to-A missense mutationleading to the substitution of tyrosine for cysteine atamino acid position 282 of the protein product(C282Y).7C282Y homozygotes account for 80%-85%of typical patients with are two other regu-larly identified mutations, one in which aspartate is sub-stituted for histidine at amino acid position 63 (H63D),and the other in which cysteine is substituted for serineat amino acid position 65 (S65C). These are generallynot associated with iron loading unless seen with C282 Yas a compound heterozygote, C282Y/H63D or C282Y/S65C (Fig.)
5 1). Over the last 10 years, mutations of othergenes coding for iron regulatory proteins have beenimplicated in inherited iron overload syndromes ( ,hepcidin, hemojuvelin, transferrin receptor 2, and ferro-portin). These are thought to account for most of thenon-HFEforms of the advent of genetic testing in the late 1990s,HFE-related HH is now frequently identified inasymptomatic probands and in presymptomatic rela-tives of patients who are known to have the , a genetic Diagnosis can be applied to indi-viduals who have not yet developed any phenotypicexpression. Therefore, these individuals have a geneticsusceptibility to developing iron overload but maynever do so, for reasons that are still to be ,10-12 This observation has changed the way wethink about hemochromatosis . Twenty years ago, itwas considered that all individuals who were geneti-cally susceptible would ultimately have evidence ofphenotypic expression. Now, it is clear that phenotypicexpression only occurs in approximately 70% ofC282Y homozygotes, and fewer than 10% of C282 Yhomozygotes will develop severe iron overload accom-panied by organ damage and clinical manifestations ,12 This acknowledgment has ledto a recognition of the different stages and progressionof hemochromatosis identified at a consensus confer-ence of the European association for the Study ofLiver Diseases in stages are defined asfollows: Stage 1 refers to those patients with the genetic dis-order with no increase in iron stores who have geneticsusceptibility.
6 Stage 2 refers to those patients with the genetic dis-order who have phenotypic evidence of iron overloadbut who are without tissue or organ damage. Stage 3 refers to those individuals who have thegenetic disorder with iron overload and have iron depo-sition to the degree that tissue and organ damage organizational schema is important to allowclinicians to categorize patients who have positivegenetic test of Iron OverloadThe current classification of iron overload syn-dromes divides patients into three groups (Table 2):(1) those who have inherited causes of iron overload,(2) those who have various causes of secondary ironoverload, and (3) a small miscellaneous 85%-90% of patients who have inher-ited forms of iron overload are homozygous for theC282Y mutation inHFE, with a small minority whoare compound heterozygotes, meaning that one allelehas the C282Y mutation and one allele has the H63 Dor the S65C mutation. The remaining 10%-15% ofpatients who have inherited forms of iron overloadmost likely have mutations in one of the otherTable 1.
7 Grading of Recommendations, Assessment,Development, and Evaluation (GRADE)Strength ofRecommendationCriteriaStrong (1)Factors influencing the strength of the recommendationincluded the quality of the evidence, presumedpatient-important outcomes, and costWeak (2)Variability in preferences and values, or more is made with less certainty, or highercost or resource consumptionQuality ofEvidenceCriteriaHigh (A)Further research is unlikely to change confidence in theestimate of the clinical effectModerate (B)Further research may change confidence in the estimateof the clinical effectLow (C)Further research is very likely to impact confidence onthe estimate of clinical effectFig. 1. Schematic representation of the protein product of the protein is extracellular. There is a short cytoplasmic tailand three extracellular alpha loops. The three principal mutations , Vol. 54, No. 1, 2011 BACON ET AL. 329aforementioned genes involved in iron of secondary iron overload are divided betweenthose causes related to iron loading anemias, thoserelated to chronic liver disease, transfusional iron over-load, and miscellaneous causes.
8 Oral iron ingestiondoes not lead to iron overload except in geneticallypredisposed individuals or those who have inherited forms of iron overload, classified asnon HFE-related HH, are juvenile hemochromatosisand iron overload resulting from mutations in thegenes for transferrin receptor 2 (TfR2), or ferroportin(SLC40A1).9 Juvenile HH is characterized by rapidiron accumulation. Mutations in two different genes(hemojuvelin and hepcidin) have been shown to causetwo forms of juvenile more commonmutation occurs in the hemojuvelin (HJV) gene onchromosome in the hepcidin gene(HAMP) also produce a form of juvenile HH, but thisis much less is a 25 amino acidpeptide produced in the liver that down-regulates ironabsorption. Mutations in theTfR2gene produce anautosomal recessive form of HH that is clinically simi-lar toHFE-related mutations may causeabnormal iron sensing by hepatocytes, which is thepredominant site of TfR2 expression. The distributionof excess iron is similar to that inHFE-related HH,namely, primarily in hepatic parenchymal autosomal dominant form of HH results fromtwo categories of mutations in the gene for the irontransporter protein, ferroportin.
9 Loss-of-function mutations decrease the cell surface localization of ferro-portin, thereby reducing its ability to export ,18 The result is iron deposition primarily in macrophages,and this disorder is called ferroportin disease . Thesecond category of mutation includes gain-of-func-tion ferroportin mutations that abolish hepcidin-induced ferroportin internalization and degradation18;distribution of iron is similar toHFE-related HH,concentrating predominantly in parenchymal iron overload occurs primarily in sub-Saharan Africa and is now considered to be the resultof a non HFE-related genetic abnormality that can beexacerbated by dietary iron individu-als with African iron overload drink an iron-rich fer-mented beverage, but iron overload can also occur inpeople who do not drink this of Secondary Iron Overload and Miscella-neous who absorb excessiveamounts of iron as a result of an underlying defectother than any of the previously mentioned inheriteddisorders have secondary iron mostcommon causes of secondary iron overload are individ-uals with ineffective erythropoiesis, parenteral ironoverload, and liver disease.
10 Individuals who receiveblood transfusions and who have transfusional or par-enteral iron overload should be distinguished fromthose who have other causes of secondary iron over-load. Parenteral iron overload is always iatrogenic, inthat blood or iron (given parenterally) must be orderedby a health care provider prior to its individuals with ineffective erythropoiesis whohave decreased utilization of iron by the bone marrowalso have transfusional iron overload because of arequirement for , it has been found that neonatal hemochro-matosis is actually a form of congenital alloimmunehepatitis with subsequent iron thesecases, immune-mediated liver injury in the fetus isassociated with the development of iron of intravenous immunoglobulin duringpregnancy slows or prevents the development of rare miscellaneous disorders includecongenital atransferrinemia and 2. Classification of Iron Overload SyndromesHereditary HemochromatosisHFE-relatedC282Y/C282YC28 2Y/H63 DOtherHFEmutationsNon HFE-relatedHemojuvelin (HJV)Transferrin receptor-2 (TfR2)Ferroportin (SLC40A1)Hepcidin (HAMP)African iron overloadSecondary Iron OverloadIron-loading anemiasThalassemia majorSideroblasticChronic hemolytic anemiaAplastic anemiaPyruvate kinase deficiencyPyridoxine-responsive anemiaParenteral iron overloadRed blood cell transfusionsIron dextran injectionsLong-term hemodialysisChronic liver diseasePorphyria cutanea tardaHepatitis CHepatitis BAlcoholic liver diseaseNonalcoholic fatty liver diseaseFollowing portocaval shuntDysmetabolic iron overload syndromeMiscellaneousNeonatal iron overloadAceruloplasminemiaCongenital atransferrinemia330 BACON ET , July 2011 PathophysiologyThere are four main categories of pathophysiologicalmechanisms of HH that should be mentioned.