Transcription of ESPEN guidelines on artificial enteral nutrition ...
1 Clinical nutrition (2005)24, 848 861 CONSENSUS STATEMENTESPEN guidelines on artificial enteralnutrition Percutaneous endoscopic gastrostomy(PEG)Chr. Lo sera, , G. Aschlb, buternec, Mathus-Vliegend,M. Muscaritolie, Y. Nivf, H. Rollinsg, P. Singerh, SkellyiaMedical Department, Rotes Kreuz Krankenhaus Kassel, 34121 Kassel, GermanybMedical Department, AKH Wels, 4600 Wels, AustriacGI nutrition , Archet 2 Hospital, 06202 Nice, FrancedDepartment of Gastroenterology, Academic Medical Centre, University of Amsterdam, The NetherlandseDepartment of Clinical Medicine, University La Sapienza , Rome, ItalyfDepartment of Gastroenterology, Rabin Medical Center, Tel Aviv University, IsraelgNutrition Nurse Specialist, Luton and Dunstable Hospital, Luton LU4 0DZ, UKhGeneral Intensive Care Department, Rabin Medical Center, Petah Tiqwa 49100, IsraeliDerbyshire Royal Infirmary, Derby DE 1 2 QY, UKReceived 23 June 2005; accepted 23 June 2005 IntroductionSince the first published report of a percutaneousendoscopic gastrostomy (PEG) in 1980 by Gaudererand Ponsky,1the procedure has been modified andimproved several times.
2 It has now replaced thesurgical gastrostomy (Witzel gastrostomy, Stammgastrostomy, Janeway gastrostomy) which wasassociated with a markedly higher rate of ,3 Placement of a PEG/PEJ (percutaneousendoscopic jejunostomy) tube is simple, safe andwell-tolerated by ,5 There is a wide rangeof diets and nutrient preparations suitable for tubefeeding currently available. Modern PEG tubesystems made of polyurethane or silicone rubberare easy to insert and well-tolerated. Clinicianshave a broad spectrum of low risk, practicable,patient-orientated forms of enteral nutritionaltherapy available. PEG-feeding, therefore, hasrapidly spread to become routine practice world-wide and is currently the method of choice formedium- and long- term enteral studies have provided new information onthe benefits and drawbacks of PEG-feeding. Wehave a clearer appreciation of ethical issuessurrounding artificial enteral feeding. Since westarted placing percutaneous enteral tube systemsby endoscopic techniques nearly 25 years ago1ourattitude towards this method has changed in manyways: in the early days PEG-tubes were often usedin patients in the advanced state of predominantlymalignant diseases; this is now regarded as aninappropriate indication in most cases being toolate to offer adequate clinical benefits to thepatients in terms of nutritional status and quality oflife.
3 Data from a large number of $ - see front Corresponding author. Tel.: +49 561 3086441;fax: +49 561 (Chr. Lo ser).published clinical studies has modified our views ona variety of issues: on the benefits and disadvan-tages of the PEG feeding; on more distinct clinicalindications with regard to important outcomeparameters ( maintenance and improvementof nutritional status and quality of life); on ethicalaspects; and on contraindications, for example inpatients with advanced dementia or during term-inal stages of incurable diseases. In many ways ourmodern point of view has shifted towards an earlierindividual consideration of additional supplemen-tary feeding via PEG tube in appropriate patients,when special nutritional advice and supplementarydrinks are not issued by various specialist authoritieshave been modified in the light of recentlypublished clinical studies and the recommendedprocedures have been markedly simplified in 9 With this background, ESPEN asked amultidisciplinary group (nutritionists, gastroenter-ologists, nurses, and medical practitioners) withspecial expertise in the field to prepare guidelinesand a consensus report on current clinical aspectsof artificial enteral nutrition via PEG-tubes in adultsand children.
4 In the following, matters relevant toclinical practice are summarized and discussed onthe basis of the currently available tube systemsIn general, tube systems for artificial enteralnutrition can be placed by nasal insertion, guidedpercutaneous application, or surgical superiority of percutaneously placed gastros-tomies compared to former surgical gastrostomyprocedures ( Witzel, Stamm, Janeway techni-que) has been shown clearly in many ,3If it is to be expected that the patientwill require artificial enteral nutrition for a longerperiod after abdominal surgery, it is advisable toprepare for subsequent jejunal feeding by prepara-tion of a fine needle catheter jejunostomy (NCJ)towards completion of the surgical procedure. Thisintraoperative technique enables the use of clini-cally effective early postoperative enteral nutritionin patients who are not able to eat sufficientamounts for a prolonged period after majorabdominal surgery. Today, various techniques andmodifications are 12 Several studies compared the various clinicaleffects of PEG tube feeding and feeding vianasogastric 17 While nasogastric tubefeeding was found to have a higher rate ofdiscomfort and complications (irritations, ulcera-tion, bleeding, dislocation, clogging)
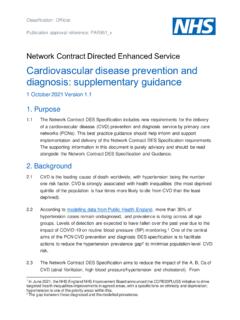
5 , PEG feedingproved to have higher subjective and socialacceptance, being less stigmatizing, and hadreduced rates of oesophageal reflux and 17 Interestingly it was clearly shownthat with regard to nutritional efficacy PEG feedingwas superior ,17 Therefore, in our presentunderstanding, feeding via PEG should be preferredif it can be expected that the patient s nutritionalintake is likely to be inadequate and supplementaryartificial enteral nutrition is necessary for a periodexceeding 2 3 1shows the decisiontree that can be used in clinical practice to selectthe tube system for enteral nutrition most appro-priate to the requirements of the individual from research with parents suggests thatdecision making in children is difficult and emo-tionally laden; there is a special need for informa-tion and individual support in these , besides the standard endoscopicprocedure, many modifications and other techni-ques for adequate percutaneous placement ofenteral tube systems were established and provenin clinical practice.
6 In the hands of an experiencedendoscopist it should be possible to place percuta-neous tube systems in nearly all cases either byendoscopic, laparoscopic, sonographic, or fluoro-scopic means. The gastric and jejunal tube systemscurrently available for enteral feeding are outlinedinFig. 2. Artificial enteral nutrition should eitherbe given into the stomach or beyond the ligamentof Treitz, there are no medical reasons for any kindof duodenal feeding. In cases in which endoscopicinsertion of a tube is not technically possible,gastric (PLG) and jejunal (PLJ) enteral tubesystems can also be placed using laparoscopicARTICLEINPRESSno riskof aspirationriskof aspirationnasojejunaltubeno longer possibleno longer adequateshort - termunknown durationlong - term( > 2 - 3 weeks )no surgeryno surgerysurgeryPEGPEJJET-PEGprolonged requirementnasogastraltubeno riskof aspirationriskof aspirationORAL nutrition :NCJF igure 1 Decision tree for the selection of the appro-priate tube system for enteral nutrition (for explanation,see text).
7 ESPEN guidelines on artificial enteral 20In those rare situations in whichthere is a stenosis of the oesophagus which isresistant to bougienage and prevents passage of anendoscope, a gastric or jejunal feeding tube can beinserted with the aid of sonographic21,22or fluoro-scopic22 24guidance. Once a stable stoma hasformed at least 4 weeks after insertion of the PEGsystem, a changeover to use of a button systemmay be conducted for cosmetic reasons, at therequest of the 28 Although, primarilyplaced button procedures are published in theliterature,29,30it is generally recommended thatbuttons are placed secondarily after initial PEGplacement with a mature established stoma button systems are much more expensive andhave to be routinely exchanged approximatelyevery 6 months because of material fatigue whichis not necessary for PEG-tubes these systems areusually only indicated for cosmetic reasons insocially fully integrated younger patients. In casesof gastroduodenal motility problems, pyloric ste-nosis or aspiration, a jejunal catheter can beplaced through the PEG and endoscopically guidedfurther into the jejunum beyond the ligament ofTreitz (JET PEG, jejunal tube PEG ) or a PEJ can beperformed as the initial 33 Tubedysfunction and the need for reinterventions aresignificantly lower in direct PEJ compared toJET PEG, therefore direct PEJ should be preferedif long-term jejunal feeding is indicated.
8 There areconflicting data in the recent literature aboutwhether or not jejunal feeding via PEJ or JET PEGdefinitely reduces the rate of reflux and 35 IndicationsAs a general rule, PEG feeding should be consideredif it is expected that the patient s nutritional intakeis likely to be qualitatively or quantitativelyinadequate for a period exceeding 2 3 weeks. Priorto the insertion of an enteral feeding tube, eachcase should be considered on its own merits, takinginto account the clinical situation, diagnosis,prognosis, ethical issues, the expected effect onthe patient s quality of life and the patient s 41 The central question to be answered iswhether PEG feeding is likely to improve ormaintain the patient s quality of life? Percutaneousinsertion of an enteral feeding tube should not be aterminal or even symbolic measure in patients withan unfavourable prognosis or an incurable diseaseand is according to our present knowledge andunderstanding very rarely indicated in patientswith short-life expectancy or advanced of a PEG-tube should always be formedical reasons and not for administrative con-venience saving time, money or manpower noris a PEG tube a substitute for good nursing considerations have to be taken intoaccount before the placement of PEG-tubes:decision-making should always be individualizedrather than the result of a general 41 Itis important to try supplementary oral nutrition byspecial drinks and individual nutritional and swal-lowing advice first.
9 But if this does not stabilize orimprove the patients situation additional enteralnutrition via PEG should be considered early inongoing diseases in order to stop the deteriorationof the nutritional status and consecutively tostabilize and even improve individual quality primary aim of enteral tube feeding is toavoid further loss of body weight, to correctsignificant nutritional deficiencies, to rehydratethe patient, to promote growth in children withgrowth retardation, and to stop the relateddeterioration of the quality of life of the patientdue to inadequate oral nutritional intake. With thisaim in view, the range of indications for the use of aPEG tube is 8,42,43 Oncological disorders(stenosing tumours in theear, nose and throat region or the upperARTICLEINPRESSPEGNCJPSJPSGPLGPLJPEJ STOMACHJEJUNUMB uttontubetubenasogastricnasojejunallapar oscopicallysurgicallysonographicallyfluo roscopicallyendoscopicallyjejunal tubePFGPFJS tamm Witzel, Figure 2 General techniques and modified methods ofplacement of enteral tube systems for gastric and jejunalnutrition: PEG, Percutaneous Endoscopic Gastrostomy;PLG, Percutaneous Laparoscopic Gastrostomy; PSG,Percutaneous Sonographically Guided Gastrostomy;PFG, Percutaneous Fluoroscopically Guided Gastrostomy;PEJ, Percutaneous Endoscopic Jejunostomy; JET-PEG,Jejunal Tube PEG; PLJ, Percutaneous Laparoscopic Jeju-nostomy; NCJ, Fine Needle Catheter Jejunostomy; PSJ,Percutaneous Sonographically Guided Jejunostomy; PFJ, Per-cutaneous Fluoroscopically Guided Lo ser et tract.)
10 PEG tubes may be usedpalliatively in inoperable cases or placed prior tosurgery, radiotherapy or chemotherapy andremoved when the patient has recovered andhas a reliable and adequate oral intake). Neurological disorders(dysphagic states aftercerebrovascular stroke or craniocerebral trau-ma, and in patients with cerebral tumours,bulbar paralysis, Parkinson s disease, amyo-trophic lateral sclerosis, cerebral palsy). Other clinical conditions(wasting in AIDS, shortbowel syndrome, reconstructive facial sur-gery, prolonged coma, polytrauma, Crohn0s dis-ease, cystic fibrosis, chronic renal failure, con-genital abnormalities, tracheo-oesophagealfistula).Another indication for use of a PEG system is thepalliative drainage of gastric juices and secretionsin the small intestine in the presence of a chronicgastrointestinal stenosis or ileus. In non-selectedpatients less than 40% of patients with a PEG tubehave a malignant underlying tothe recent literature, the main therapeutic indica-tions are benign neurological disorders (almost 50%of cases) and ENT disorders usually malignant(approximately 30% of cases).