Transcription of Exploring Alcohol’s Effects on Liver Function
1 N association between Liver disease and heavy alcoholconsumption was recognizedmore than 200 years ago (Smart andMann 1992). Long-term heavy alco-hol use is the most prevalent singlecause of illness and death from liverdisease in the United States (NationalCenter for Health Statistics 1994).The Liver is particularly susceptible toalcohol-related injury because it is theprimary site of alcohol alcohol is broken down in theliver, a number of potentially danger-ous by-products are generated, such asacetaldehyde and highly reactivemolecules called free radicals. Per-haps more so than alcohol itself, theseproducts contribute to alcohol-inducedliver Liver is one of the largest or-gans in the body; it has not only con-siderable reserves but also the abilityto regenerate itself. Consequently,symptoms of Liver damage may notappear until damage to the organ isquite extensive. Epidemiologicalstudies suggest that a threshold doseof alcohol must be consumed forserious Liver injury to become appar-ent (Mezey et al.)
2 1988). For men, thisdose amounts to 600 kilograms (kg)taken chronically over many years, anintake that can be achieved by con-suming approximately 72 ounces (oz)of beer, 1 liter of wine, or 8 oz dis-tilled spirits ( , 5 6 standarddrinks1) daily for 20 years. For wom-en, the threshold dose is one-fourth toone-half that amount. In this article,the phrase heavy drinking refers tothis daily long-term alcohol consump-tion clearly plays a major role in thedevelopment of alcohol-related liverdamage. Yet, no more than one-half ofheavy drinkers develop alcoholic hep-atitis or cirrhosis (French et al. 1993).This finding suggests that other fac-tors heredity, environment, or both interact to influence the course of liverdisease. This article examines sometypes of Liver injury and their potentialmechanisms, discusses factors that mayplace people at increased risk for suchinjury, and provides a brief descriptionof different treatment 21, NO.
3 1, 19975 Exploring Alcohol sEffects on Liver Function JACQUELYNJ. MAHER, large proportion of heavy drinkers develop serious alcoholic Liver to alcoholic hepatitis and cirrhosis appears to be influenced byheredity, gender, diet, and co-occurring Liver illness. Most alcoholic Liver damage isattributed to alcohol metabolism. Liver injury may be caused by direct toxicity ofmetabolic by-products of alcohol as well as by inflammation induced by these by-products. Exposure of Liver cells to bacterial toxins may contribute to Liver Liver injury can lead to fibrosis and, ultimately, to cirrhosis. Increasedunderstanding of the mechanisms of Liver injury has led to innovative treatments foralcoholic Liver disease, including the use of corticosteroids, antioxidants, antibiotics,and certain polyunsaturated fats. KEY WORDS: heavy AOD use; alcoholic Liver cirrhosis;alcoholic hepatitis; ethanol metabolism; biochemical mechanism; toxic drug effect;inflammation; drug therapy; hereditary factors; gender differences; diet; risk factors;endotoxin; fibrosis; free radicals; etiology; literature review1 One standard drink is defined as 12 fluidounces (oz) of beer, 5 fluid oz of wine, or oz of distilled MAHER, , is associ-ate professor of medicine, Universityof California, San Francisco, work was funded by grants fromthe National Institute on AlcoholAbuse and Alcoholism (NIAAA)(AA00215 and AA07810) and theAlcoholic Beverage MedicalResearch OFALCOHOL-INDUCEDLIVERDAMAGEA lcohol-related Liver damage can bedivided into three categories (Frenchet al.)
4 1993): Fatty Liver . Some degree of fat depo-sition in the Liver occurs in almost allheavy drinkers. It also may occurtransiently in nonalcoholics after asingle drinking session. Fatty Liver isreversible and is not believed to leadto more serious damage. Alcoholic hepatitis. This disorder ischaracterized by widespread in-flammation and destruction ( ,necrosis) of Liver tissue. Scar tissuemay begin to replace healthy livertissue, a process called of alcoholic hepatitismay include fever, jaundice,2andabdominal pain. The condition canbe fatal but may be reversible withabstinence. Alcoholic hepatitisoccurs in up to 50 percent of heavydrinkers (National Institute onAlcohol Abuse and Alcoholism[NIAAA] 1993). Alcoholic cirrhosis. This most ad-vanced form of Liver disease is diag-nosed in 15 to 30 percent of heavydrinkers. Between 40 and 90 percentof the 26,000 annual deaths fromcirrhosis are alcohol related (Dufouret al.
5 1993). A cirrhotic Liver is char-acterized by extensive fibrosis thatstiffens blood vessels and distorts theinternal structure of the Liver . Thisstructural damage results in severefunctional impairment, which maylead secondarily to malfunction ofother organs, such as the brain andkidneys. Although alcoholic cirrhosisis usually fatal because of complica-tions ( , kidney failure and hyper- tension in the vein carrying blood tothe Liver [ , the portal vein]), it canstabilize with , these three conditionshave been considered sequentiallyrelated, progressing from fatty Liver toalcoholic hepatitis to cirrhosis. How-ever, heavy drinkers may developalcoholic cirrhosis without first devel-oping hepatitis. Moreover, alcoholichepatitis may have a sudden onset anda rapid course, causing death beforecirrhosis can OFALCOHOLAn understanding of alcohol metab-olism provides the basis for under-standing alcohol-induced liverdamage.
6 Most of the alcohol thatpeople drink is metabolized in theliver. The major pathway for alcoholmetabolism involves the enzymealcohol dehydrogenase (ADH). Thisenzyme converts alcohol to acetalde-hyde through a chemical processcalled oxidation. (For more informa-tion on the metabolism of alcohol, seethe article by Bode, pp. 76 83.) As alcohol is brokendown in the Liver , anumber of potentiallydangerous by-productsare is highly toxic to thebody, even in low concentrations. Nor-mally, however, the enzyme aldehydedehydrogenase (ALDH) rapidly oxi-dizes acetaldehyde to acetate. Most ofthe acetate travels through the blood-stream to other parts of the body, whereit can enter other metabolic cycles(Lieber 1994) that produce energy oruseful molecules. The usual biologicalrole of both ADH and ALDH is to metab-olize vitamin A ( , retinol).The microsomal enzyme oxidizingsystem (MEOS) is an alternate path-way for alcohol metabolism in theliver.
7 Microsomal enzymes belong toa family of proteins called cytochromes, located in a cellu-lar substructure called the endoplas-mic reticulum (see figure in glossary,pp. 93 96), detoxify harmful sub-stances that enter the body. TheMEOS oxidizes alcohol to acetalde-hyde by means of a cytochrome calledP450 2E1, or CYP2E1, which is foundin the endoplasmic reticulum of livercells. Normally functioning at a lowlevel, CYP2E1 is stimulated ( ,induced) to a higher level by the pres-ence of alcohol. Thus, the MEOS becomes increasingly important asalcohol consumption becomes heavierand more mechanisms that influence liverinjury are both poorly understood andcontroversial. Moreover, they interact incomplex ways. The following sectionsbriefly discuss aspects of these mecha-nisms and their of OxygenOxygen-related factors that influencealcohol-induced Liver damage includethe Effects of free radicals, antioxi-dants, and of the direct celldamage that occurs during alcoholicliver disease is believed to be causedby free radicals.
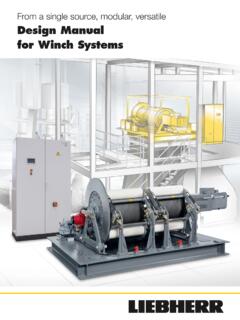
8 Free radicals arehighly reactive molecular fragmentsthat frequently contain oxygen. Smallquantities of free radicals are pro-duced as normal by-products of vari-ous metabolic processes. Thesefragments are quickly scavenged bynatural protective molecules in thecell, called antioxidants ( , glu-tathione and vitamins A and E). How-ever, when free radicals are producedin excess or when antioxidant defensesare impaired, the free radicals mayinteract destructively with vital cellconstituents, potentially causing deathof the RESEARCHWORLD3An enzyme called catalase also can convertalcohol to acetaldehyde. However, this enzymerarely plays an important role in humans andwill not be discussed further in this article(Lieber 1994).2 For definitions of this and other technicalterms, see glossary, pp. 93 21, NO. 1, 19977 Alcohol s Effects on Liver FunctionThe Liver is the largest organ of thebody, weighing pounds. It occu-pies the upper right and part ofthe left section of the fibrous tissue divides theliver into functional units calledlobules, cylindrical structures sev-eral millimeters (mm) in length to 2 mm in diameter.
9 The hu-man Liver contains 50,000 to100,000 a microscopic level, eachlobule is nourished by blood thatenters from the blood vessels at theperiphery (see figure). These ves-sels include small branches of thehepatic artery as well as branchesof the portal vein, which bringsnutrients and other dissolved sub-stances from the intestine. Bloodfrom these peripheral vessels enterschannels called sinusoids, where itbathes all the cells in the lobulebefore exiting through a vein locat-ed in the center of the lobule. Thesinusoids are lined in part byKupffer cells, immune-system cellsthat attack and engulf bacteria andforeign matter in the blood (seeDiehl 1993 for more information).The unidirectional transport ofblood within lobules from theperipheral vessels to the centralvein significantly affects liverfunction and disease. The regionadjacent to the peripheral vessels isreferred to as zone 1, and the cellssurrounding the central vein makeup zone 3.
10 Between these zoneslies zone 2. Blood flowing throughthe sinusoids releases dissolvedsubstances, including oxygen,mostly to zone 1 and in the leastamount to zone 3. In cirrhoticlivers, the relative lack of oxygen( , hypoxia) in zone 3 appears toencourage fibrosis in that functions of the Liver areessential to life. As the metaboliccrossroads of the body, the liverfilters circulating blood, removingand destroying toxic substances. Itsecretes bile into the small intes-THELIVER STRUCTURE ANDFUNCTION tine to help digest fats and renderthem soluble for absorption. Nutrientsare carried from the small intestinethrough the portal vein directly to theliver, which then synthesizes choles-terol, metabolizes or stores sugars,processes fats, stores vitamins, andassembles proteins for use within theliver or elsewhere. The Liver alsoconverts the products of proteinmetabolism into urea for excretion bythe kidneys. In addition, it regulatesblood-clotting mechanisms.