Transcription of Fibular (Peroneal) Neuropathy - University of Washington
1 Fibular ( peroneal ) NeuropathyElectrodiagnostic Features and Clinical CorrelatesChristina Marciniak,MDINTRODUCTIONF ibular or peroneal Neuropathy is the most frequent mononeuropathy encountered inthe lower limb and the third most common focal Neuropathy encountered overall, aftermedian and ulnar ,2 Following revised anatomic terminology publishedin 1998, the peroneal nerve is also now known as the Fibular nerve, to prevent confu-sion of this nerve with those regions with similar is another term for thefibula and, thus, this revised terminology for this nerve, its branches, and relatedmusculature is based on language describing the both Fibular andperoneal are considered acceptable terms, Fibular and it related terminology ispreferred and therefore will be used throughout this of ankle dorsiflexion and the resultant foot drop are common presentationsof Fibular Neuropathy , but may also be seen in a wide variety of other clinical conditions,including sciatic mononeuropathy, lumbosacral plexopathy, or a lumbar (L) 5 Disclosures: No relevant of Physical Medicine and Rehabilitation, Northwestern University , Feinberg Schoolof Medicine, The Rehabilitation Institute of Chicago, 345 East Superior, Chicago, IL 60611, USAE-mail Fibular peroneal Neuropathy ElectrodiagnosticKEY POINTS Fibular ( peroneal ) Neuropathy is the most common mononeuropathy encountered in thelower limbs.
2 Clinically, sciatic mononeuropathies, radiculopathies of the 5th lumbar root, and lumbosa-cral plexopathies may present with similar findings of ankle dorsiflexor weakness, thusevaluation is needed to distinguish these disorders. The most common site of injury to the Fibular nerve is at the Fibular head. The deep Fibular branch is more frequently abnormal than the superficial branch. Electrodiagnostic studies are useful to determine the level and type (axonal, demyelin-ating) of injury. The presence of any compound muscle action potential response on motor nerve conduc-tion studies, recorded from either the tibialis anterior or extensor digitorum brevis, is asso-ciated with good long-term Med Rehabil Clin N Am 24 (2013) 121 137 $ see front matter 2013 Elsevier Inc. All rights Additionally, ankle dorsiflexion weakness may be the initial presentationof generalized disorders, such as amyotrophic lateral sclerosis, or a hereditary retrospective series of 217 patients presentingwith paresisor paralysis of footdorsiflexors, of whom 68% had peripheral nerve abnormalities as the cause of theirweakness, 31% had weakness related to a common Fibular nerve lesion,30%an L5 rad-iculopathy, and 18% due to a neuropathies may also presentwith predominantly sensory symptoms limited to the distribution of the deep or super-ficial Fibular nerve or its addition to documenting Fibular nerve abnormali-ties and the level of the injury, electrodiagnostic techniques have also been used toassess the potential for recovery of nerve ,7 ANATOMYC ommon Fibular ( peroneal )
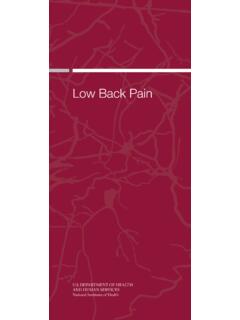
3 NerveThe common Fibular ( peroneal ) nerve is derived from the lateral division of the sciaticnerve. Fibers from the dorsal fourth and fifth lumbar, as well as the first and secondsacral nerve roots, join with tibial axons to form the sciatic nerve (Fig. 1). Though boundin the nerve sheath with the tibial nerve in the thigh, the Fibular and tibial axons are sepa-rate even within the sciatic nerve at this the thigh, a branch arises from thefibular division of the sciatic nerve to innervate the short head of the biceps bifurcation of the sciatic nerve in the distal thigh at the superior poplitealfossa, the common Fibular nerve travels along the lateral side of the fossa at the borderof the biceps femoris muscle to the lateral knee. At this level, the nerve gives offa branch, the lateral cutaneous nerve of the calf, which supplies sensation to the upperthird of the anterolateral leg.
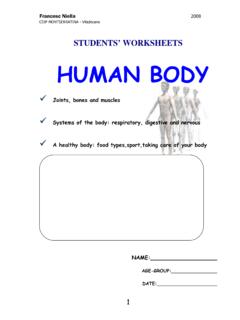
4 The sural communicating branch of the lateral sural cuta-neous nerve joins with the medial sural cutaneous nerve to form the sural nerve. Thecommon Fibular nerve then travels superficially at the lateral fibula and is located about1 to 2 cm distal to the Fibular head before entering the anterior compartment of the legwhere it divides into deep and superficial branches at the Fibular head (Fig. 2).Deep Fibular ( peroneal ) NerveThedeepfibular (Peroneal) nervesuppli esmotorinnervationtoallanteriorcompartme ntmuscles (the tibialis anterior, the extensor digitorum longus, and extensor hallucis lon-gus) and the fibularis tertius, also known as the peroneus tertius. The anterior tibialis isthe strongest foot dorsiflexor, although the extensor digitorum longus and the fibularistertius assist with this deep Fibular nerve travels distally in the calf and atthe level of the ankle joint, fascia overlying the talus and the navicular bind the deepfibular nerve dorsally.
5 Ventrally, the extensor hallucis longus muscle fibers and tendonand the inferior extensor retinaculum overlay the nerve. The inferior extensor retinac-ulum is a Y-shaped band anterior to the ankle; the anterior tarsal tunnel is consideredthe space located between the inferior extensor retinaculum and the fascia overlyingthe talus and navicular. Just rostral or under the inferior extensor retinaculum, thedeep Fibular nerve branches into medial and lateral branches. The lateral branch ofthe deep Fibular nerve travels under the extensor retinaculum, as well as the extensordigitorum and hallucis brevis muscles to innervate these muscles and nearby undertheextensor hallucisbrevistendon to supplysensationto the skin between the first and second Fibular ( peroneal ) NerveThe superficial Fibular (or peroneal ) nerve arises from the common Fibular nerve in theproximal leg and travels distally in the leg through the lateral compartment.
6 AfterMarciniak122 Fig. nerve: anatomy. Netter illustration Elsevier Inc. All rights ( peroneal ) Neuropathies123 Fig. peroneal nerve and branches: anatomy. Netter illustration Elsevier Inc. All rights muscular innervation to the fibularis (peroneus) longus and brevis muscles inthe lateral compartment of the leg, the terminal sensory branch supplies sensation tothe lower two-thirds of the anterolateral leg and the dorsum of the foot, except for thefirst web space. It becomes superficial within the muscular compartment about 5 cmabove the ankle joint where it pierces the fascia to become subcutaneous. It dividesinto its two terminal sensory branches, the intermediate and medial dorsal cutaneousnerves. The intermediate dorsal cutaneous nerve travels to the third metatarsal spaceand then divides into the dorsal digital branches to supply sensation to the lateral twodigits.
7 The medial dorsal cutaneous branch passes over the anterior aspect of theankle overlying the common extensor tendons, runs parallel to the extensor hallucislongus tendon, and divides distal to the inferior retinaculum into three dorsal Fibular ( peroneal ) NerveA common anatomic variant, the accessory Fibular ( peroneal ) nerve, may be identifiedin the performance of studies to the extensor digitorum generally arises fromthe superficial Fibular nerve as it courses under the fibularis brevis muscle, travelingdistally to the foot posterior to the lateral subsequently branches toinnervate ligaments, joints, and the extensor digitorum brevis muscle. Prevalence asa normal anatomic variant has been reported to be 17% to 28% in anatomic studiesand 12% and 22% ,11 13 CAUSESF ibular neuropathies are most often traumatic in origin; stretch or compression isa common feature in the history (Box 1).
8 14,15 Recurring external pressure at the fibularhead may result in this complication, such as that seen in patients at bed rest or in indi-viduals who habitually cross their compression of the superficial and/or deep Fibular nerves has also been described, such as that occurring from fascialbands or intraneural Fibular neuropathies located at the Fibular head may be found in the setting ofrecent weight loss, frequently in conjunction with a history of leg ,18 20 Fibularnerve palsies were reported in prisoners of war during World War II who lost from 5 to11 another case series, it was noted that 20% of 150 cases of Fibular mononeur-opathy were associated with dieting and weight mean weight decrease inthese patients was kg, with most patients having moderate to severe weaknessof foot dorsiflexion and has been theorized that loss of subcutaneous fatleads to increased susceptibility of the nerve to compression at this associated with weight loss most often demonstrates conduction blockon electrodiagnostic testing, with the severity correlating with clinical recently Fibular Neuropathy has been described following bariatric trauma around the knee or ankle may result in Fibular nerve injuries due tothe nerve s proximate and superficial locations at the level of these joints.
9 Lacerationsfrom saws, boat propellers, or lawn mowers have all been surpris-ingly, those with nerve in continuity have better recovery of function. Knee disloca-tions, particularly open, rotatory, or posterolateral corner injuries can results inproximal Fibular nerve Fibular nerve abnormalities may be local-ized following spiral Fibular requiring external fixation of theankle may result in more distal , in the case of fractures, it hasbeen noted that Fibular Neuropathy may be localized to the Fibular head electrodiag-nostically, though the fracture is an alternative ( peroneal ) Neuropathies125 Box 1 Fibular ( peroneal ) Neuropathy : reported causesKnee or Fibular head Anaphylactoid purpura Arthroplasty (knee) Arthroscopy (Knee) Baker cyst Bed rest Birth trauma Boney exostoses Casts Crossed-leg sitting Cryotherapy Fractures (femur, tibia, Fibular ) Fibrous arch Foot boards Ganglion Gun shot wounds Heterotopic ossification Hematoma Hemangiomas Intravenous infiltration or injections Knee dislocation Knee stabilization by helicopter pilots Kneepads Kneeling Lacerations Lipoma Knee surgery Schwannoma Sequential compression devices Sesamoid bone of the lateral head of gastrocnemius Severe valgus or varus deformity at the knee Splints Squatting (childbirth, strawberry picking, farm workers)
10 Synovial cysts Traction Varicose vein surgery Venous thrombosis Water ski kneeboardsMarciniak126 Although the most common site of injury following surgical procedures is at thefibular head, focal Fibular neuropathies have also been reported at the level of thecalf, ankle, and foot. Following total knee replacements, Fibular nerve abnormalitiesmay present with sensory symptoms or decreased range of tibial osteotomies, done in association with Fibular osteotomies, Fibular nerveabnormalities have been noted in 2% to 27% of 32 The abnormalities of ankleand toe extension and the sensory loss described following these procedures arethought to result from hardware placement, tourniquet effects, or the Fibular abnormalities as the result of surgeries may be subclinical. In 11 casesstudied prospectively with electrophysiologic testing, pre- and post-osteotomysurgery, abnormalities were present postoperatively in 27%, though only one patientwas clinically Neuropathy is the most common lower limb mononeuropathy encountered ,34 Common or proximal deep Fibular nerve injuries at or near the level of thefibular head are most often found, particularly in football or soccer players, and may beseen in isolation or in association with severe ligamentous knee injuries or ,34 Some athletes reporting pain and weakness in a Fibular nerve distributionhave been found to have constriction of the nerve by the fibularis longus or chronic exertional compartment syndrome may also result in foot drop andshould be considered.