Transcription of Full/Modified Trauma Activation Orders
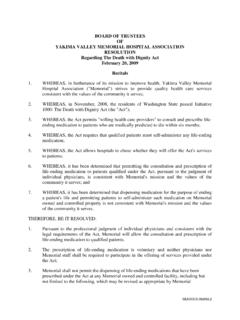
1 R*PO0001*rPO0001 Full/Modified TraumaActivation OrdersRev. 3-09 Form 0819 Page 1 of 1 Full/Modified Trauma Activation Orders full Trauma Activation Shock (Hypotension) - Systolic BP <90 (Age 15-Adult) - Systolic BP <80 (Age 0-14) GSW (Head, Neck, Torso, or Groin) Compromised airway or ventilation Traumatic cardiac arrest Traumatic Amputation (Arm/Leg) Page Trauma Surgeon: Time paged_____Called Back_____ Page Trauma Team: Time paged_____ modified Trauma Activation Significant CNS injury (GCS <10 or paralysis) Stab wound to the torso Flail chest Multiple long bone fractures Crush injury to pelvis Ejection from vehicle Auto vs. Pedestrian >10mph or thrown > 10 feet Any patient not meeting the criteria who decompensates in the ED Page Trauma Team: Time paged_____ Page Trauma Surgeon: Time paged_____Called Back_____Scene Information:Radio___ Telephone ___ AgencyCalling_____ Date: _____ Time of Call _____Location _____ETA: _____Procedures: = Mandatory = Optional 2 16 gauge or larger IV s with LR (if possible) Oximetry ECG Vital signs every 15 minutes Foley catheter (if no blood at meatus) NG tube (OG if Facial fractures)Patient Information:Male____ Female____ Age___BP____ / ____ Pulse_____ Resp Rate_____GCS_____Rhythm_____Intubated___ __IV_____Description of Accident / Mechanism of InjuryLab Orders .
2 CBC Repeat H&H (#1)_____ BMP INR/PTT (head injuries GCS<10) (#2)_____ ABG (if intubated) Blood alcohol level UA by dipstick Urine drug screen Band & Hold Crossmatch _____ units---Stay ahead_____units HCG (if female 13-50 yrs.) Other: Drug & Etoh Intervention, (CRM order ) Rehab notificationRadiography: Chest X-Ray C-Spine (if blunt Trauma ) Pelvis (if blunt Trauma ) Thoracic Spine L/S Spine Extremity: OtherCT: Head Neck Chest Abdomen/PelvisPhysician s Signature:_____Date/Time:_____SpecialtyP agedCalled BackArrived No Activation Physicians preferencePerson receiving TransmissionYAKIMA valley Trauma SERVICESREHABILITATION CONSULTATION FOR TRAUMAThe Trauma Rehab Coordinator is notified BY FAX, for EACH Trauma Team activationAND any head injury, spinal cord injury, significant peripheral nerve injury and majorextremity REHAB CONSULTATIONDate of Trauma :Type of Trauma : full modified Non-activationHospital: Yakima Regional Yakima valley MemorialDiagnosis:Disposition: Admitted to (room number): OR Home Transferred to.
3 FAX TO:(509) 225-3059 Rehab Admission Coordinator/ Trauma ManagerOffice: (509) 573-3482, Cell: (509) 728-4045 Yakima valley Trauma ServicesRehabilitation ConsultationRev. 1-09 Form 1103 Page 1 of 1r*PO0001*rPO0001