Transcription of Functional Family Therapy
1 Department of JusticeOffice of Justice ProgramsOffice of Juvenile Justice and Delinquency PreventionJohn J. Wilson, Acting AdministratorFrom the AdministratorWhile a number of States andcommunities are turning to punitiveapproaches to addressing juvenilecrime, research indicates that suchapproaches, despite their high cost,are largely ineffective. Juvenile offen-ders removed from their families andcommunities eventually return, andunless their underlying behavioralproblems have been treated effectively,these problems are likely to contributeto further Family Therapy (FFT)draws on a multisystemic perspectivein its Family -based prevention andintervention efforts. The program ap-plies a comprehensive model, proventheory, empirically tested principles,and a wealth of experience to thetreatment of at-risk and Bulletin chronicles FFT s evolu-tion over more than three decades;sets forth the program s core prin-ciples, goals, and techniques; andreviews its research implementation of FFTis described, and an example ofeffective replication is years of clinical researchindicate that FFT can prevent theonset of delinquency and reducerecidivism at a financial and humancost well below that exacted by thepunitive approaches noted believe this Bulletin will help youto consider the program s meritsfor your J.
2 WilsonActing AdministratorDecember 2000ineffective and costly. By removing adoles-cents from their families and communities,punitive programs inadvertently make ado-lescents problems more difficult to solvein the long run. Regardless of how adoles-cents problems manifest themselves, theyare complex behavioral problems embed-ded in adolescents psychosocial systems(primarily Family and community). Thus, Family -based interventions that adopt amultisystemic perspective are well suitedto treating the broad range of problemsfound in juveniles who engage in delin-quent and criminal Family Therapy (FFT) is afamily-based prevention and interventionprogram that has been applied successfullyin a variety of contexts to treat a range ofthese high-risk youth and their families. Assuch, FFT is a good example of the currentgeneration of Family -based treatments foradolescent behavior problems (Mendel,2000; Sexton and Alexander, 1999). It com-bines and integrates the following elementsinto a clear and comprehensive clinicalmodel: established clinical theory, empiri-cally supported principles, and extensiveclinical experience.
3 The FFT model allowsfor successful intervention in complex andmultidimensional problems through clinicalpractice that is flexibly structured and cul-turally sensitive and also accountable toyouth, their families, and the TherapyThe Office of Juvenile Justice and Delin-quency Prevention (OJJDP) is dedicated topreventing and reversing trends of increaseddelinquency and violence among adoles-cents. These trends have alarmed the publicduring the past decade and challenged thejuvenile justice system. It is widely acceptedthat increases in delinquency and violenceover the past decade are rooted in a num-ber of interrelated social problems childabuse and neglect, alcohol and drug abuse,youth conflict and aggression, and earlysexual involvement that may originatewithin the Family structure. The focus ofOJJDP s Family Strengthening Series is toprovide assistance to ongoing efforts acrossthe country to strengthen the Family unit bydiscussing the effectiveness of Family inter-vention programs and providing resourcesto families and arising from juvenile crime are aserious concern for many local communi-ties.
4 Expressions of adolescent behaviorproblems range from minor offenses ( ,curfew violations and trespassing) to seri-ous crimes ( , drug abuse, theft, andviolence) and result in staggering personal,economic, and social costs. Until recently,most communities were left on their ownto determine how to address juvenilecrime, and many communities turned toexclusively punitive approaches such asincarceration. Mounting evidence, how-ever, indicates that such approaches areFamilyStrengtheningSeriesThomas L. Sexton and James F. Alexander2 Although commonly used as an interven-tion program, FFT is also an effective pre-vention program for at-risk adolescentsand their families. Whether implementedas an intervention or a prevention pro-gram, FFT may include diversion, proba-tion, alternatives to incarceration, and/orreentry programs for youth returning tothe community following release from ahigh-security, severely restrictive institu-tional on the results of extensive indepen-dent reviews, FFT has been designatedvariously as a blueprint program (Alex-ander et al.)
5 , 2000), an exemplary model program (Alexander, Robbins, and Sexton,1999), and a Family based empiricallysupported treatment (Alexander, Sexton,and Robbins, 2000). These designationsreflect FFT s 30 years of clinical andresearch experience and its use at a widerange of intervention sites in the UnitedStates and other targets youth between the ages of 11and 18 from a variety of ethnic and cul-tural groups. It also provides treatmentto the younger siblings of referred adoles-cents. FFT is a short-term intervention including, on average, 8 to 12 sessions formild cases and up to 30 hours of directservice ( , clinical sessions, telephonecalls, and meetings involving communityresources) for more difficult cases. Inmost cases, sessions are spread over a3-month period. Regardless of the targetpopulation, FFT emphasizes the impor-tance of respecting all Family members ontheir own terms ( , as they experiencethe intervention process).Data from numerous studies of FFT out-comes suggest that when applied as in-tended, FFT reduces recidivism and/orthe onset of offending between 25 and60 percent more effectively than otherprograms (Alexander et al.
6 , 2000). Otherstudies indicate that FFT reduces treat-ment costs to levels well below those oftraditional services and other interven-tions (Alexander et al., 2000). As FFT hasevolved, it has adopted a set of guidingprinciples, goals, and techniques thatcan be used even when resources arelimited for example, in managed careand similar contexts that restrictopen-ended and non-outcome-basedresource Evolution ofFunctional FamilyTherapyMore than 30 years ago, it became appar-ent to FFT progenitors that although therate and severity of juvenile delinquency,violence, and drug abuse were growing ata frightening pace, intervention programsremained seriously underdeveloped(Alexander and Parsons, 1973). In 1969,researchers at the University of Utah sPsychology Department Family Clinic de-veloped FFT to serve diverse populationsof underserved and at-risk adolescentsand their families. These populationslacked resources, were difficult to treat,and often were perceived by helping pro-fessionals as not motivated to these underserved populationswere diverse in terms of Family organiza-tion, relational dynamics, presentingproblems, and cultures, they often shareda common factor: They had entered theschool counseling, mental health, or juve-nile justice systems angry, hopeless, and/or resistant to developers of FFT recognized thatsuccessful treatment of these populationsrequired service providers who were sen-sitive to the needs of these diverse fami-lies and competent to work with them,and who understood why the families hadtraditionally resisted treatment.
7 Over thepast 30 years, FFT providers have learnedthat they must do more than simply stopbad behaviors; they must motivate fami-lies to change by uncovering Family mem-bers unique strengths, helping familiesbuild on these strengths in ways that en-hance self-respect, and offering familiesspecific ways to its development, FFT has been adynamic clinical system. It has retainedits core principles while adding clinicalfeatures that improve successful out-comes in the diverse communities inwhich it has been implemented. Morethan two decades ago, FFT began focusingon therapist characteristics and in-sessionprocesses from an integrated perspectivethat combines research and practice. Thisperspective, in turn, has contributed tothe training of therapists for subsequentinterventions by identifying specific step-by-step interventions and their impact onyouth and other Family the late 1990 s, FFT further articulatedits clinical change model by refining thephases of intervention (Sexton andAlexander, 1999; see table), developinga systematic approach to training andprogram implementation, and adding acomprehensive system of client, process,and outcome assessment.
8 The systemis implemented through a computer-based client tracking and monitoringsystem known as the Functional FamilyTherapy Clinical Services System (FFT CSS). This most recent iteration of FFThelps clinicians identify and implementgoals for therapeutic change in a way thatpromotes accountability through processand outcome evaluation. As a result, FFThas matured into a clinical interventionmodel that includes systematic training,supervision, process, and outcome as-sessment components all directed atimproving the delivery of FFT in Principles, Goals,and TechniquesFunctional Family Therapy is so named toidentify the primary focus of intervention(the Family ) and reflect an understandingthat positive and negative behaviors bothinfluence and are influenced by multiplerelational systems ( , are Functional ).FFT is a multisystemic prevention pro-gram, meaning that it focuses on the mul-tiple domains and systems within whichadolescents and their families live. FFT isalso multisystemic and multilevel as anintervention in that it focuses on thetreatment system, Family and individualfunctioning, and the therapist as majorcomponents.
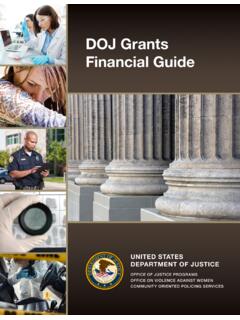
9 Within this context, FFTworks first to develop Family members inner strengths and sense of being able toimprove their situations even if mod-estly at first. These characteristics pro-vide the Family with a platform for changeand future functioning that extends be-yond the direct support of the therapistand other social systems. In the long run,the FFT philosophy leads to greater self-sufficiency, fewer total treatment needs,and considerably lower the level of clinical practice, FFT in-cludes a systematic and multiphaseintervention map Phase Task Analysis that forms the basis for responsive clini-cal decisions. This map gives FFT a flex-ible structure by identifying treatmentstrategies with a high probability of suc-cess and facilitating therapists clinicaloptions. FFT s flexibility extends to allfamily members and thereby results ineffective moment-by-moment decisions in3 Functional Family Therapy Clinical Model: Intervention Phases Across TimeEngagement and MotivationBehavior ChangeGeneralizationEarlyMiddleLateSourc e: Sexton and Alexander, negativity, dropout Family motivation and blaming (risk).
10 Hopelessness (risk).Lack of motivation (risk).Credibility (protective).Alliance (protective).Treatment availability(protective).Behavior ( , presentingproblem and risk and protec-tive factors).Relational problems sequence( , needs/functions).Context (risk and protectivefactors).Interpersonal skills (validation,positive interpretation,reattribution, reframing, andsequencing).High availability to goalsDevelop and implementindividualized change presentingdelinquency relational skills ( ,communication andparenting).Poor parenting skills (risk).Negativity and blaming (risk).Poor communication (risk).Positive parenting skills(protective).Supportive communication(protective).Interpersonal needs (dependson context).Parental pathology (dependson context).Developmental level (dependson context).Quality of relational skills(communication, parenting).Compliance with behaviorchange problem (session focusing).Change plan community resourcesnecessary to support relationships with school/community (risk).