Transcription of Guideline: Newborn baby assessment (routine)
1 maternity and NeonatalClinical GuidelineQueensland Health Clinical Excellence Queensland Newborn baby assessment (routine) Queensland Clinical Guideline: Newborn baby assessment (routine) Refer to online version, destroy printed copies after use Page 2 of 25 Document title: Newborn baby assessment (routine) Publication date: November 2021 Document number: Document supplement: The document supplement details development processes and implementation activities, and is integral to and should be read in conjunction with this guideline. Amendments: Full version history is supplied in the document supplement. Amendment date: November 2021 Replaces document: Author: Queensland Clinical Guidelines Audience: Health professionals in Queensland public and private maternity and neonatal services Review date: November 2026 Endorsed by: Queensland Clinical Guidelines Steering Committee Statewide maternity and neonatal Clinical Network (Queensland) Contact: Email: URL: Disclaimer This guideline is intended as a guide and provided for information purposes only.
2 The information has been prepared using a multidisciplinary approach with reference to the best information and evidence available at the time of preparation. No assurance is given that the information is entirely complete, current, or accurate in every respect. The guideline is not a substitute for clinical judgement, knowledge and expertise, or medical advice. Variation from the guideline, taking into account individual circumstances, may be appropriate. This guideline does not address all elements of standard practice and accepts that individual clinicians are responsible for: Providing care within the context of locally available resources, expertise, and scope of practice Supporting consumer rights and informed decision making, including the right to decline intervention or ongoing management Advising consumers of their choices in an environment that is culturally appropriate and which enables comfortable and confidential discussion.
3 This includes the use of interpreter services where necessary Ensuring informed consent is obtained prior to delivering care Meeting all legislative requirements and professional standards Applying standard precautions, and additional precautions as necessary, when delivering care Documenting all care in accordance with mandatory and local requirements Queensland Health disclaims, to the maximum extent permitted by law, all responsibility and all liability (including without limitation, liability in negligence) for all expenses, losses, damages and costs incurred for any reason associated with the use of this guideline, including the materials within or referred to throughout this document being in any way inaccurate, out of context, incomplete or unavailable. Recommended citation: Queensland Clinical Guidelines. Newborn baby assessment (routine). Guideline No. 26. Queensland Health. 2021. Available from: State of Queensland (Queensland Health) 2021 This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives International licence.
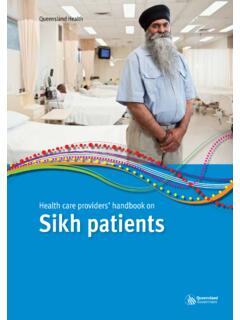
4 In essence, you are free to copy and communicate the work in its current form for non-commercial purposes, as long as you attribute Queensland Clinical Guidelines, Queensland Health and abide by the licence terms. You may not alter or adapt the work in any way. To view a copy of this licence, visit For further information, contact Queensland Clinical Guidelines, RBWH Post Office, Herston Qld 4029, email For permissions beyond the scope of this licence, contact: Intellectual Property Officer, Queensland Health, GPO Box 48, Brisbane Qld 4001, email Cultural acknowledgement We acknowledge the Traditional Custodians of the land on which we work and pay our respect to the Aboriginal and Torres Strait Islander Elders past, present and emerging. Queensland Clinical Guideline: Newborn baby assessment (routine) Refer to online version, destroy printed copies after use Page 3 of 25 Flow Chart: Routine Newborn baby assessment Flowchart: Indications for further investigation and/or urgent follow-up are not exhaustive.
5 Use clinical judgementReview discharge criteria Observations, feeding, output Vitamin K Hepatitis B vaccinationDiscuss If < 24 hours of age, when to seek urgent medical assistance Routine screening ( hearing, NBST, pulse oximetry) Childhood immunisation program Support agencies Newborn care Health promotion Medications as indicated Personal Health Record (red book) Referral and follow-upo Routine 5 7 days & 6 weeksDischargeFamily centred care Consider cultural needs Discuss with parents: purpose, process, timing and limitations of assessments Ask about parental concerns Encourage participationTiming Initial exam immediately after birth and any resuscitation Full and detailed assessment within 48 hours and always prior to discharge Follow-up 5 7 days and 6 weeks If unwell/premature stage as clinically indicatedReview history Maternal medical/obstetric/social and family Current pregnancy Labour and birth Sex, gestational age, Apgar scores and resuscitation Since birth medications, observations, feeding Environment consider: Warmth, lighting Correct identification Infection control precautions PrivacyEquipment prepare.
6 Overhead warmer if required Stethoscope Ophthalmoscope Tongue depressor & glove Pencil torch Tape measure, infant scales, growth charts Pulse oximeter Documentationo Infant Personal Health Record o Medical recordo neonatal clinical pathwayPreparationAssessmentGeneral appearance Skin colour, integrity, perfusion State of alertness Activity, range of spontaneous movement Posture, muscle toneGrowth status Chart head circumference, length, weight on centile chartsHead, face, neck Head shape, size Scalp, fontanelles, sutures Eye size, position structure Nose, position, structure Ear position, structure Mouth, palate, teeth, gums tongue, frenulum Jaw sizeShoulders, arms, hands Length, proportions, symmetry Structure, number of digitsChest Size, shape, symmetry, movement Breast tissue, nipples Heart sounds, rate, pulses Breath sounds, resp rate Pulse oximetry Abdomen Size, shape, symmetry Palpate liver, spleen, kidneys UmbilicusGenitourinary Male penis, foreskin, testes Female clitoris, labia, hymen Anal position, patency Passage of urine and stoolHips, legs, feet Ortolani and Barlow s manoeuvres Leg length, proportions, symmetry and digitsBack Spinal column, skin Symmetry of scapulae, buttocksNeurological Behaviour, posture Muscle tone, spontaneous movements Cry Reflexes Moro, suck, graspDiscuss Document Refer Discuss findings with parents Document in health record(s) Refer as indicatedFurther investigation UrgentGrowth and appearance Dysmorphic features Excessive weight loss Jaundice < 24 hours of age Central cyanosis Petechiae new/unrelated to birth Pallor, haemangiomaHead and neck Enlarged/bulging/sunken fontanelle Macro/microcephaly Subgaleal haemorrhage Caput, cephalhaematoma Fused sutures Facial palsy/asymmetry on crying Hazy, dull cornea.
7 Congenital cataract Absent red eye reflex Pupils unequal/dilated/constricted Purulent conjunctivitis/yellow sclera Nasal obstruction Dacryocyst; cleft lip/palate Unresponsive to noise Absent ear canal or microtia Ear drainage Small receding chin/micrognathia Neck masses, swelling, webbing Swelling over or fractured clavicleUpper limbs Limb hypotonia, contractures, palsy Palmar crease patternChest Respiratory distress Apnoeic episodes Abnormal HR, rhythm, regularity Heart murmurs Weak or absent pulses Positive pulse oximetryAbdomen Organomegaly Gastrochisis/exomphalos Bilateral undescended testes Bilious vomiting Inguinal hernia Signs of umbilical infectionGenitourinary No urine/meconium in 24 hours Ambiguous genitalia Testicular torsion Hypospadias, penile chordee micropenis, hydroceleHips, legs and feet Risk factors for hip dysplasia Positive/abnormal Barlow s and/or Ortolani manoeuvres Contractures/hypotonia Talipes Developmental hip dysplasiaBack Curvature of spine Non-intact spine Tufts of hair/dimple along intact spineNeurological Weak/irritable/absent cry Absent/exaggerated reflexes No response to consoling Seizures Altered state of consciousness Urgent follow-up; GP: general practitioner.
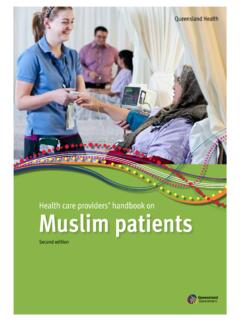
8 HR: heart rate, NBST: Newborn screening test, SUDI: sudden unexpected death in infancy, <: less than Queensland Clinical Guideline: Newborn baby assessment (routine) Refer to online version, destroy printed copies after use Page 4 of 25 Flow Chart: Management of Newborn baby during pulse oximetry screening for CCHD Flowchart: Manage as abnormal (positive) screenPulse oximetry screening Ensure baby is fed/settled Apply neonatal oxygen saturation sensor(s) to either foot or right hand and either foot Connect sensor(s) to motion tolerant pulse oximeter(s) Keep sensor insitu until trace is steady (< one minute) Record highest SpO2 and if used calculate difference between hand and foot readingsNoYesPulse oximetry screen for CCHDBaby 24 hours of age? Screen immediately prior to dischargeo May result in false positive Follow local protocols for screening by home visiting midwife or GPYesNoRepeat screen normal? Admission to neonatal unito Consider investigations for sepsis, other respiratory/vascular problems If respiratory distress or cardiac signso SpO2 and cardio-respiratory monitoring Consider CXR, 4 limb BP, echocardiography Delay discharge If baby is well, repeat screen in 3 4 hours Contact RSQ as requiredRespiratory distress: Tachypnoea > 60/min Grunting Chest recessionCardiac signs: Bradycardia < 60bpm Tachycardia > 160 bpm Poor femoral pulses Cardiac murmurAbnormal (positive)Abnormal (borderline) Discharge as usual Review by MO or NNP Repeat screen in one hour Requires urgent medical review Admit to neonatal unit Commence close clinical surveillance SpO2 and cardio-respiratory monitoring Investigate for sepsiso Refer to QCG EOGBS guideline Investigate for CCHD Consider investigations for other respiratory/vascular problems Contact RSQ as requiredNoYesNormal (negative)Repeat screen normal?
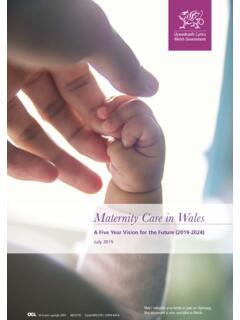
9 CCHD: critical congenital heart disease; BP: blood pressure, bpm: beats per minute, CXR: chest X-ray, EOGBS: early onset Group B Streptococcus, GP: general practitioner; HR: heart rate, min: minute, MO: medical officer, NNP: neonatal nurse practitioner, QCG: Queensland Clinical Guidelines, RSQ: Retrieval Services Queensland, SpO2: oxygen saturation, >: greater than; : greater than or equal to; <: less than; less than or equal to Queensland Clinical Guideline: Newborn baby assessment (routine) Refer to online version, destroy printed copies after use Page 5 of 25 Flow Chart: Pulse oximetry screening of Newborn baby for critical congenital heart disease Flowchart: Between 24 36 hours of age measure oxygen saturation in foot or RH OR RH and either foot NEGATIVE screen Continue normal carePOSITIVE screen Urgent medical review Consider differential diagnosis Repeat screen in 1 hour Consider differential diagnosis Repeat screen in 1 hour90 94% in foot or RHOR > 3% difference between RH and foot?
10 90 94% in foot or RHOR > 3% difference between RH and foot?YesYesNoNoYesYesYes 95% foot or RHor 95% foot AND 3% difference between RH and foot?90 94% foot or RHor > 3% difference between RH and foot?< 90% foot or RH?RH: right hand, >: greater than; :greater than or equal to; <: less than; : less than or equal to Queensland Clinical Guideline: Newborn baby assessment (routine) Refer to online version, destroy printed copies after use Page 6 of 25 Flow Chart: Newborn bloodspot screening test Flowchart: Repeat screening indicated?Completion: Add relevant clinical information Complete baby s personal health record (red book) Follow local procedures for dispatching screening card to laboratory Repeat screening: Repeat screen at appropriate time Note reason for repeat on screening cardo If 10% glucose note time and date ceasedNoYesIndicationTime of repeatAt birth: Complete screening card o Identification of babyo Identification of mothero Baby s UR numbero Birth weighto GestationTiming: Collect sample at 48 72 hours of age If discharged from hospital before 48 hours of age:o Discuss option for collection ( by home visiting midwife, child health nurse)Feeding note on card: Type, date and time of first milk feed If not feeding (NBM) If baby fed within last half hourSampling technique.