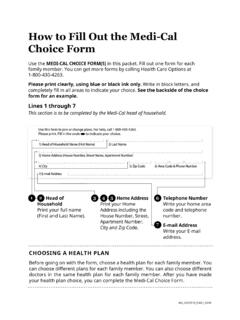
Transcription of Health Plan Choice Form
1 --STEP 2: Choose your Health plan : Applicant's Signature Date OR Authorized Representative Signature (if any) DateHealth plan Choice FormUse this form to join or change a Health plan . For FREE help with this form , contact Health Care Options at 1-844-580-7272. Mail completed form to california department of Health Care Services, Health Care Options, Box 989009, West Sacramento, CA 95798-9850. Please print clearly using blue or black ink. STEP 1: Tell us about yourself:Combine my Medicare and Medi-Cal benefits in one plan . Choose one of these Cal MediConnect plans:Keep my Medicare separate AND choose a Medi-Cal Managed Care plan .
2 Choose one of these Medi-Cal Managed Care plans to get your Medi-Cal benefits:Confidential_0004073_ENG_0219 Doctor/Clinic Code:Doctor/Clinic Code:STEP 3: Read the important information on the back before signing. I understand that by filling out and signing this form , I am choosing how to get my Health care. (optional)(optional)ORCHOICE ACHOICE BFirst Name Last NameAddressCity Zip Code (Area Code) Phone NumberDate of Birth Due Date (if pregnant) Social Security Number////--MaleFemaleSex:PACE plan :Program of the All-Inclusive Care for the Elderly (PACE): You may qualify for PACE (see instructions).
3 If you want to get your Medicare and Medi-Cal benefits combined in a PACE plan , fill out this option in addition to Choice A or B. If you do not qualify, you will get your care through the Choice A or Choice B plan that you chose above in Step 052 AltaMed Senior BuenaCare 060 Brandman Cent for Sen Care 074 Pacific PACE 076 LA Coast PACE 817 Blue Shield Promise 818 Anthem 801 Health Net 800 Care 816 Molina Dual Options 352 Health Net Comm Solutionso HN Health Net Comm Solutionso MO Molina Healthcare Partner 304 Care Health Plano BC Anthem Blue Cross Partnrshpo BL Blue Shield Promiseo KA KP Cal, LLCo LA Care Health plan , ,HCOOMBA, ,HCOOMBASTEP 2.
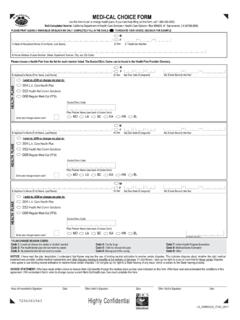
4 Choose your Health plan :Applicant's Signature Date OR Authorized Representative Signature (if any) DateHealth plan Choice FormUse this form to join or change a Health plan . For FREE help with this form , contact Health Care Options at 1-844-580-7272. Mail completed form to california department of Health Care Services, Health Care Options, Box 989009, West Sacramento, CA 95798-9850. Please print clearly using blue or black ink. STEP 1: Tell us about yourself:Combine my Medicare and Medi-Cal benefits in one plan . Choose one of these Cal MediConnect plans:Keep my Medicare separate AND choose a Medi-Cal Managed Care plan .
5 Choose one of these Medi-Cal Managed Care plans to get your Medi-Cal benefits:Confidential_0004073_ENG_0219 Doctor/Clinic Code:Doctor/Clinic Code:STEP 3: Read the important information on the back before signing. I understand that by filling out and signing this form , I am choosing how to get my Health care. (optional)(optional)ORCHOICE ACHOICE BFirst Name Last NameAddressCity Zip Code (Area Code) Phone NumberDate of Birth Due Date (if pregnant) Social Security Number////- -MaleFemaleSex:PACE plan :Program of the All-Inclusive Care for the Elderly (PACE): You may qualify for PACE (see instructions).
6 If you want to get your Medicare and Medi-Cal benefits combined in a PACE plan , fill out this option in addition to Choice A or B. If you do not qualify, you will get your care through the Choice A or Choice B plan that you chose above in Step 052 AltaMed Senior BuenaCare 060 Brandman Cent for Sen Care 074 Pacific PACE 076 LA Coast PACE 817 Blue Shield Promise 818 Anthem 801 Health Net 800 Care 816 Molina Dual Options 352 Health Net Comm Solutionso HN Health Net Comm Solutionso MO Molina Healthcare Partner 304 Care Health Plano BC Anthem Blue Cross Partnrshpo BL Blue Shield Promiseo KA KP Cal.
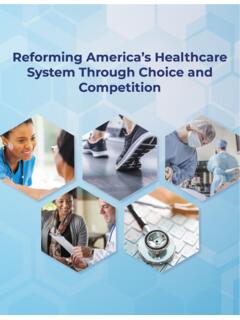
7 LLCo LA Care Health PlanPlease use the following example when you fill in the form :PLEASE PRINT IN CAPITAL LETTERS CU3 KDV4 LEW5 MFX6 NGY7 OHZ -8P9Q0R,SPrivacy StatementThe department of Health Care Services will keep the information you provide. It is used only to enroll and/or disenroll people that are eligible for Medi-Cal managed care. The laws that allow this are in the Welfare and Institutions Code, Section , , , , , , , , 14088, 14089, , and 14631, and california Code of Regulations, Section If any information asked for on the Choice form is missing, then someone on the form may not be able to join a Health plan , get out of a plan , or choose the plan he or she wants.
8 Only other government agencies that relate to the Medi-Cal program can see the information you provide. The persons listed on the form can look at the files that Medi-Cal keeps on them. However, any information that is being used in an investigation or lawsuit cannot be seen. If you want to see your Medi-Cal file, contact the department of Health Care Services at the address on the other side of this use the following example when you fill in the form :PLEASE PRINT IN CAPITAL LETTERS CU3 KDV4 LEW5 MFX6 NGY7 OHZ -8P9Q0R,SPrivacy StatementThe department of Health Care Services will keep the information you provide.
9 It is used only to enroll and/or disenroll people that are eligible for Medi-Cal managed care. The laws that allow this are in the Welfare and Institutions Code, Section , , , , , , , , 14088, 14089, , and 14631, and california Code of Regulations, Section If any information asked for on the Choice form is missing, then someone on the form may not be able to join a Health plan , get out of a plan , or choose the plan he or she wants. Only other government agencies that relate to the Medi-Cal program can see the information you provide. The persons listed on the form can look at the files that Medi-Cal keeps on them.
10 However, any information that is being used in an investigation or lawsuit cannot be seen. If you want to see your Medi-Cal file, contact the department of Health Care Services at the address on the other side of this