Transcription of IJPUT REVIEWS AND SPECIAL ARTICLE A Review of ...
1 International Journal of Perioperative ultrasound and Applied Technologies, January-April 2012;1(1):25-2925 IJPUTA Review of ThromboelastographyREVIEWS AND SPECIAL ARTICLEA Review of ThromboelastographyMilind Thakur, Aamer B AhmedABSTRACTThis is the first of two articles describing the uses of point ofcare testing in coagulation management. The first articledescribes the basis of thromboelastography with its physicalprinciples and uses. The second describes discussions of casestudies in clinical : Point of care tests, thromboelastography ,Coagulation, to cite this ARTICLE : Thakur M, Ahmed AB. A Review ofThromboelastography. Int J Periop ultrasound Appl Technol2012;1(1) of support: NilConflict of interest: None declaredINTRODUCTIONH aemostasis in the process of clot formation is a jointfunction of platelet activation to form a platelet plug andcoagulation cascade leading to clot formation.
2 Traditionally,this function is measured using conventional tests, such asplatelet number and function, activated partialthromboplastin time, prothrombin time, thrombin time,fibrinogen levels and fibrin degradation , these test various parts of the coagulationcascade but in isolation and are static tests, which take timeto complete and invariably lead to delay in a timelymanagement. In addition to this, they need to be repeatedat intervals and although they assess platelet number, theydo not give accurate information on platelet function. Beingplasma tests, they might not be accurately reflecting whatactually happens to the (TEG) is a method of testing theefficiency of coagulation in the blood. It was first developedby Dr Hellmut Hartert at University of Heidelberg, Schoolof Medicine in 1948.
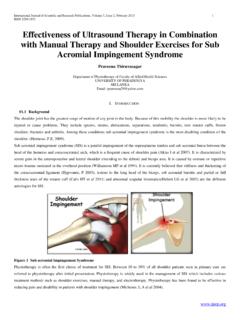
3 TEG overcomes the above-mentionedlimitations of conventional coagulation provides an effective and convenient means ofmonitoring whole blood coagulation. It evaluates the elasticproperties of whole blood and provides a global assessmentof haemostatic is recommended for and commonly used in assessinghaemostasis during liver transplantation, obstetricprocedures and cardiac surgery. It is useful not only in casesof bleeding patients but also used to predict In cardiac surgery, where the risk of bleedingis higher, TEG monitoring helps to identify and target thosewho need test sample is placed in the oscillating cup at 37 pin is suspended from torsion wire into blood sample(Fig. 1). Development of fibrin strands couple the motionof the cup to the pin. This coupling is directly proportionalto the clot strength.
4 Increased tension in the wire is detectedby the electromagnetic transducer and electrical signalamplified to create a trace, which is displayed on computerscreen. Deflection of the trace is proportional to OF MEASUREMENTr-time: Represents period of time of latency from start oftest to initial fibrin formation. This represents the standardclotting studies. Normal range: 15 to 23 minutes (nativeblood); 5 to 7 minutes (kaolin-activated).k-time: Represents time taken to achieve a certain level ofclot strength (where r-time = time zero) equates toamplitude 20 mm. Normal range: 5 to 10 minutes (nativeblood); 1 to 3 minutes (kaolin-activated). -angle: Measures the speed at which fibrin build-up andcross-linking takes place (clot strengthening), and henceassesses the rate of clot formation.
5 Normal range: 22 to38 (native blood); 53 to 67 (kaolin-activated).Maximum amplitude: MA is a direct function of themaximum dynamic properties of fibrin and platelet bondingvia GPIIb/IIIa and represents the ultimate strength of thefibrin clot and which correlates to platelet function: 80%platelets; 20% fibrinogen. normal range: 47 to 58 mm (nativeblood); 59 to 68 mm (kaolin-activated). : Basis of the thromboelastogram (TEG) Thakur, Aamer B AhmedSituations with deficient coagulation factors, such ashypofibrinogenaemia, thrombocytopenia or thrombo-cytopathy show prolonged r and k times and decreased MAand hypercoagulable states, k and r times are decreasedwith an increase in MA and index (CI)A mathematical formula determined by the manufacturer,which takes into account the relative contribution of eachof these four values into one equation.
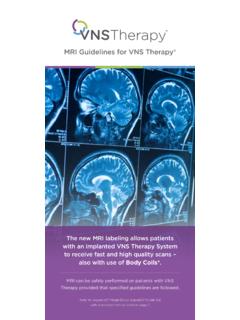
6 CI (normal range 3 to 3 mm) is an overall indicator of coagulation andindicates normal, hypo- or hypercoagulable : This is percentage decrease in amplitude 30 minutespost-MA and gives measure of degree of fibrinolysis(Fig. 2). Normal range < (native blood); < (celite-activated) and similarly, LY60 is the percentage decreasein amplitude 60 minutes (A60)Amplitude at 30 (60) minutes computer prediction of 30 minutes lysis basedon interrogation of actual rate of diminution of traceamplitude commencing 30 seconds post-MA and is theearliest indicator of abnormal EPL > LY30 (30 mins EPL = LY30)Normal EPL < 15%Fibrinolysis leads to LY30/ LY60 EPL and A30/ INTERPRETATION OF DIFFERENTSTAGES OF COAGULATION BY TEG Clot formation Clotting factors r, k times Clot kinetics Clotting factors r, k times Platelets MA Clot strength/stability Platelets MA Fibrinogen Reopro-mod MA Clot resolution Fibrinolysis LY30/60.
7 EPL A30 ModificationsEach thromboelastograph has two sets of curette-pin-transducer. Up to eight channels may be connected to thecomputer. So, each evaluation may be simultaneouslyperformed in different channels with the addition ofactivators, plasma, platelet concentrate, heparinase,antifibrinolytics, and titrated protamine, aiming not onlyat coagulopathy diagnosis but also at testing the treatmentin evaluation of clot formationduring heparinisation ( cardiopulmonary bypass) is nowavailable. Heparinase (an enzyme breaking heparin) hasbeen introduced to the TEG(r) technology, assisting inidentification of abnormal coagulation in heparinised patients, prior to heparin reversal with protamine. This isuseful during long pump runs, deep hypothermia and useof ventricular assist devices or complicated major vascularcases such as thoracoabdominal aneurysm.
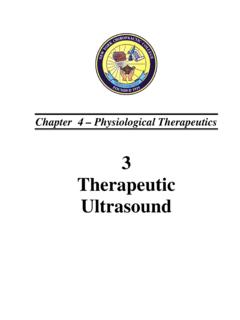
8 The test will alsohelp us to decide, if more protamine is needed to fullyreverse heparin (Fig. 3).Other antifibrinolytic agents, such as Epsilon-aminocaproic acid, tranexamic acid and aprotinin (still hasa role in liver transplant, though use in cardiac surgery inquestion due to postoperative renal failure) can be added totest their effectiveness in treatment of c7E3 Fab (Reopro), which binds to the plateletGPIIb/IIIa receptors, will eliminate platelet function fromthe thromboelastogram. The MA will become a function offibrinogen activity (MAR). Platelet function can then becalculated by subtracting MAR from the whole blood thromboelastometry uses a modification of TEG,signal of the pin is transmitted using an optical detectorinstead of a torsion wire. Movement orginates from pin andnot the cup.
9 The ROTEM uses an electronic pipette, whichimproves reproducibility and performance. In ROTEM, thesensor shaft rotates rather than the cup. The ROTEM technology avoids several limitations of traditionalinstruments for thromboelastography , especially thesusceptibility to mechanical shocks and , TEG is rated as the best compromise betweenusability, usefulness and cost as compared to ROTEM2(Fig. 4).Fig. 2: A typical TEG traceInternational Journal of Perioperative ultrasound and Applied Technologies, January-April 2012;1(1):25-2927 IJPUTA Review of ThromboelastographyPLATELET FUNCTION ANALYSISP ersonalised antiplatelet therapy is possible with TEG. TEGanalysis provides the measure of maximum platelet function,and hence the degree of hypercoagulability and extent ofinhibition needed.
10 The platelet mapping assay reports thepercent inhibition and net platelet function. So, you canidentify Whether patients are resistant to antiplatelet therapy The effect of the therapy Whether they are at their therapeutic level Their risk for ischaemic or bleeding aggregometry is also an alternative test but it ismore laboratory based rather than point of USES OF THROMBOELASTOGRAPHYT hromboelastography is mainly used in the following: Cardiac surgery Liver transplantation Major obstetric Surgery and TEGThe main reasons for bleeding in cardiac surgery patientscan be classified under four broad headings of preoperativefactors, cardiopulmonary bypass (CPB) factors, post-CPBfactors and surgical bleeding. Preoperative factors includeantiplatelet medications, such as aspirin/clopidogrel, patientson warfarin/heparin and pre-existing clotting or plateletabnormalities.