Transcription of Interpreting pulmonary function tests: Recognize the ...
1 866 CLEVELAND CLINIC JOURNAL OF medicine VOLUME 70 NUMBER 10 OCTOBER 2003HE MAJOR LIMITATIONof pulmonaryfunction tests is in how they are inter-preted. They can be used to identify the pat-tern and severity of a physiologic abnormali-ty, but used alone, they generally cannot dis-tinguish among the potential causes of , pulmonary function tests must beinterpreted in the context of a proper history,physical examination, and ancillary diagnostictests. Once a pattern is recognized (obstruc-tive, restrictive, or normal) and its severitymeasured, that information, combined withother patient data, often leads to a this article we will provide an overviewof basic pulmonary function tests and an algo-rithm for using and Interpreting them, andthen we use three cases to explain how to usethese tests to identify the pattern of respirato-ry dysfunction, thenmake the pulmonary function TESTINGP ulmonary function tests are ordered.
2 To evaluate symptoms and signs of lung dis-ease (eg, cough, dyspnea, cyanosis, wheez-ing, hyperinflation, hypoxemia, hypercap-nia)1,2 To assess the progression of lung disease To monitor the effectiveness of therapy To evaluate preoperative patients inselected situations1,2 To screen people at risk of pulmonary dis-ease such as smokers or people with occu-pational exposure to toxic substances inoccupational AL-ASHKAR, MDDepartment of General internal medicine ,The Cleveland ClinicREENA MEHRA, MDDepartment of pulmonary and Critical CareMedicine, University Hospitals, ClevelandPETER J.
3 MAZZONE, MD, MPHD epartment of pulmonary and Critical CareMedicine, The Cleveland ClinicInterpreting pulmonary function tests: Recognize the pattern,and the diagnosis will followREVIEWnABSTRACTWhen Interpreting pulmonary function tests, one shouldfirst try to determine the pattern of abnormality: is itobstructive, restrictive, or normal? pulmonary function testscannot by themselves distinguish among the potentialcauses of abnormalities, and must be interpreted in light ofthe patient s history, physical examination, and ancillarystudies.
4 Once a pattern is recognized, the diagnosis willoften POINTSE very clinician should have an organized approach tointerpreting pulmonary function tests that will allow him orher to Recognize and quantitate Interpreting the results, one should ascertain thatthe test was acceptable and reproducible and that thepatient s demographic data are recognition is key. A low FEV1/FVC ratio (the forcedexpiratory volume in 1 second divided by the forced vitalcapacity) indicates an obstructive pattern, whereas anormal value indicates either a restrictive or a the FEV1/FVC ratio is normal, a low forced vital capacityvalue indicates a restrictive pattern, whereas a normalvalue indicates a normal function tests are not generally indicated inpatients without symptoms, and they may be confusingwhen nonpulmonary diseases that affect the pulmonarysystem are active (eg, congestive heart failure).
5 T868 CLEVELAND CLINIC JOURNAL OF medicine VOLUME 70 NUMBER 10 OCTOBER 2003 To monitor for the potentially toxiceffects of certain drugs or chemicals (eg,amiodarone, beryllium) pulmonary function tests are notother-wise indicated in patients without symp-toms, and they may be confusing when non- pulmonary diseases that affect the pul-monary system are active (eg, congestiveheart failure).nCOMPONENTSOF pulmonary function TESTSS pirometrySpirometry is the measurement of the air mov-ing in and out of the lungs during various res-piratory allows one to deter-mine how much air can be inhaled andexhaled, and how majorlimitationof pulmonaryfunction testsis in howthey areinterpretedPULMONARY function TESTSAL-ASHKAR AND COLLEAGUESKey abbreviations and definitionsused in pulmonary function testsDLCOD iffusing capacity of the lung.
6 The capacity of the lungs to transfer carbonmonoxide (mL/min/mm Hg)DLCOcThe DLCO adjusted for hemoglobin (mL/min/mm Hg)DLVAThe DLCO adjusted for volume (mL/min/mm Hg/L)DLVCThe DLCO adjusted for both volume and hemoglobin (mL/min/mm Hg/L)ERVE xpiratory reserve volume;the maximum volume of air that can be exhaled fromthe end-expiratory tidal position (L)FETF orced expiratory time;the amount of time the patient exhales duringthe FVC maneuver (seconds)FEV1 Forced expiratory volume in 1 second;volume of air forcibly expired froma maximum inspiratory effort in the first second (L)FEV1/FVC ratioRatio of FEV1to FVCFRCF unctional residual capacity;the volume of air in the lungs following a tidalvolume exhalation = ERV + RV (L)FVCF orced vital capacity;the total volume that can be forcefully expiredfrom a maximum inspiratory effort (L)ICInspiratory capacity;the maximum volume of air that can be inhaled from tidalvolume end-expiratory level;the sum of IRV and VT (L)IRVI nspiratory reserve volume.
7 The maximum volume of air that can be inhaled fromthe end-inspiratory tidal position (L)LLNL ower limit of normal;the lowest value expected for a person of the same age,gender,and height with normal lung functionPEFPeak expiratory flow;the highest forced expiratory flow (L/second)RVResidual volume;the volume of air that remains in the lungs after maximalexhalation (L)TLCT otal lung capacity;the total volume of air in the lungs at full inhalation;the sumof all volume compartments (IC + FRC or IRV + VT+ ERV + RV) (L)TV or VTTidal volume;the volume of air that is inhaled or exhaled with each breathwhen a person is breathing at rest (L)VCVital capacity.
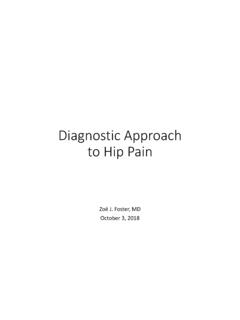
8 The maximum volume of air that can be exhaled starting frommaximum inspiration,TLC (L) can be measured either as slow vital capacity(SVC) or forced vital capacity (FVC)TABLE 1 The components of the respiratory cycleare labeled as lung volumes and lung capaci-ties (a capacity is the sum of one or more vol-umes; TABLE 1, FIGURE 1). We are mainly con-cerned with three of these measures: The forced vital capacity (FVC).Aspirometric maneuver begins with the patientinhaling as deeply as he or she can.
9 Then thepatient exhales as long and as forcefully aspossible; the amount exhaled in this manneris the FVC. The forced expiratory volume in 1 sec-ond (FEV1)is the amount of air exhaled dur-ing the first second of the FVC maneuver. Ittends to be lower in diseases that obstruct theairway, such as asthma or emphysema. The FEV1/FVC ratiois used to deter-mine if the pattern is obstructive, restrictive,or capacityThe diffusing capacity is a measure of the abil-ity of the lungs to transfer ,4 Diffusion in the lungs is most efficientwhen the surface area for gas transfer is highand the blood is readily able to accept the gasbeing transferred.
10 It is thus decreased in: Conditions that minimize the ability ofCLEVELAND CLINIC JOURNAL OF medicine VOLUME 70 NUMBER 10 OCTOBER 2003871 The three mostimportantmeasures arethe: FVC FEV1 FEV1/FVC ratioTime (sec)"Breathenormally""Breathe inas deeplyas you can""Breathe outas hard and aslong you can"Volume (L)Residualvolume (RV)Expiratoryreservevolume (RV)Tidal volume (TV)Inspiratoryreservevolume (IRV)Functionalresidualcapacity(FRC)Insp iratorycapacity (IC)Forcedvitalcapacity(FVC)Totallungcap acity(TLC)Forcedexpiratoryvolume in1 second(FEV1)1 second Lung volumes and capacitiesFIGURE volumes and capacities depicted on a volume-time most important values are the forced vital capacity (FVC)