Transcription of LATERAL PAIN SYNDROMES OF THE FOOT AND …
1 The majo rity of pa tient enco un ters with the pod iatri st aresec on dar yto pa in in the foot and/o rankl e. If we draw animag inary line bisectingthe low er leg and ext end ingdis ta lly to th e thi rd toe, pa in in the medi al aspe ct of thefoot an d ank le is typicallyst ra ight forwar d. Ther e is apre dominanceof medial heel pa in, which is usuallypla ntar fas ciitis. Medial arch sym pto msare se en fre qu ent lyin the pe s valgus foot typ e suc h has post erio r tibialte ndinit is. Less frequent ly one ma y se e tarsal tunn elsy ndrome. Fi rst ra ypa in sy nd ro mes ar ety picall yasso ciatedwit h ha llux valgus or hall ux limitus; and fina lly,deg ener ati ve jointdise ase is freq uen tly see nin th emedi alcol umn an d th e second ta rsome ta ta rsal join t. Ev aluati onand di agnosis of these dis order s ca n ty pically be do newi th out muc ha sbeen my ex pe rien ce thatpain in the lat eral foo tand an kl e presen ts challengesin clinical diagno sis.
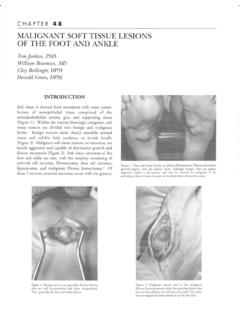
2 If on edra ws a silv er dollar sized circ le on the late ral an kle(Fi gur e 1), on e can apprec iate th e signi fi can t numbe r ofst ructur es that can be pathol ogi c, whic h are in clo sepr ox imity to one anothe r. Moreov er, one can ap pre ciatetha t ther e is ov erl ap in pot en tially pa tholo gic struc tureswhen doing a palpatoryexa mi na ti on. These stru ctu resinc lude the fibula, LATERAL ankle gutt er , LATERAL ank leliga ment s, the sinus tarsi , and the pe roneal ten do ar ea the size of you r th umb ca n enco mpass ma ny ofth ese str uc tur lly in the foo t, pa in se ems to affect the lat eral 2me ta ta rsa ls and in the re gi on of the styl oid pr oce ss of thefifth me tata rs al. When eva luatin g pa in juxta pose d to thefif th me ta ta rsa l base , one is usua lly deal ing wit h perone alten don pa th ol ogy. If the pai n is direc tly on th e stylo idpr oces s, then thi s is usu al ly what I term an insertio na lperone us bre vis tendini tis.
3 The other common area of pa inwi ll beinthe cubit al tun nel,whic hiswhe rethe peroneuslongus ten do n wi ll tra verse und er th e cu boid. Often arad iogra ph will reve al an ospe roneu th ere is painwit h palpation be tw ee n the cubo id and the fibula , thenon e shou ld be co ncer ned ab ou t pero nea l ten dinosis,es pec ially if ther e is an y ed em a in th e ar ea . Per onealte ndi nit is ma ybe no ted inthe re tro malleolar reg ion of thefib ula .Also, the synd rome of su blux ing pe rone al tendonsma y be in thi s area . St en osi ng perone al tend init is can beseen inferi or to the tip of the later al malleo lus, mor eco mmo nly seen in th e pes cavu s foo t type. pain on thedor solate ral foot ove rlying the bas es of the fourt hand fift hme ta ta rsa ls is a str ess sy ndro me tha t I te rm pe riostit is ofth eme ta ta rsa th isar ti cl e, Iwillbr eak dow nthe differe nt el em ent sof di agnosi s and tr ea tme nt.
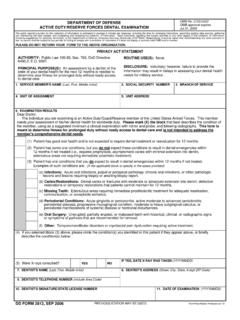
4 This inf orm at ion is base d onmy clini ca l expe rie nc e and wi ll hop ef ul ly prov ide a moresy ste ma tic wa y to appr oach pa in synd rome s of the lat eralfoot an dankle .STRESSFRACTUREOFTHEFIBULAStr ess fra ctur esofthefibul aaretypical ly se en in 2pati entpop ulat ions .Fat iguest ressfra cturesareseen in the at hl etewh o is runni ng and ins uff icien cy str ess frac tures in theol der pat ient wi th os teo por osi s. Diagn os is of th e stres sfra cture is relativel y stra igh t for war d. Ty pi cal ly, the re wi llbe signifi can t ed ema , er yt hem a, an d wa rm th over th edi sta lfibul compa re both extre mi tiesto asse ss forsub tle edem a. Pai n wi ll be no ted wi th palpat ion of th efib ula. Radi ographs wi llusual ly rev eal the st re ss fractur ,DPMCHAPTER3 Figure 1. Clinical photographdepictingthe close proximityof multipleanatomicsites. X=sinus tarsi; Y=anterior talofibularligament;arrow =impingementsite (talofibularjoint); Z= ns verse frac ture in the diaphysea l-me tap hyse al re gi onof the bone (Figure 2).
5 Mag netic resonanceimagi ng(MRI) is rare ly necessaryeven wi th an ini tia l negativeradi ogra ph. Reme mbe r, there may bea3-we ek lagperiodof onset of sym ptom s an d radi ogr aphic evi den ce of afra cture .Ty pi ca lly on subseq uen tse ria lradiog raphs, bonecallus wi ll be evid ent. Trea tme nt of th iscondi tio nincludesfr act ur e boot immobiliz ati on, com pr ession, and the fibula is a nonweight-b earing bone , and the sefra ct ure sare st able, nonweig ht bear ing isunnec ess ary. Onecan co ns ider a bo ne gr owt h stimu lator to enhance bon ehealin gespecially in th epatien twith ass ociated ris kfa ctorssuc has obesity, smoking,ost eopo ro si s, and/o rdi abet of the LATERAL ankle ligaments will gene ra lly resu ltin 2 main patie nt com pla ints cons isti ng of pain andins ta bility. Some patients on ly ha ve pain or vi ce ve rsa, an dsome pat ients will have both.
6 Ifi nd ithelpfu lto deter mi newh ich of the 2 symptomsare wor se . If inst abi lit y is thepri mar y concern,then trea tment is st raight fo rwar ming th at th e clinical ex amina tion is co nsiste nt withankl e ins tab ility, with a positive ant erior drawe r an d talarti lt tes ts , th en tr eatment will invo lve bracing tec hni que s,phys ical th erapy, and /or sur gic al repai r. Ifpain is the mainconce rn ,th en th ings are mor ediff icu lt be cause the re maybe other ca uses ofpain. MRI is helpf ul inthis scenario torul e out other cau ses of pain su ch as lat eral talaroste oc hon dra llesion ten , pat ients will hav e conc om ita nt pat holog ies ofliga me nt rup ture an d osteo chondra l lesio ns of the tal the MRI is rema rk abl e for lat eral ank le ligam entder an gem en t an d neg ati ve fo r oth er pat ho logies, thentr eat men t can be inst ituted to st ab ilize the an kleco ns erva ti vel y or with sur ger y.
7 If how ever, there is anos teoc hondra l les ion in addi tion to lig ame nt pathol ogy ,th en onehas to det er mi neifbo thar econtr ibu ti ng to pai nor one or the ot her. One th ing to co ns ider withoste oc hon dra llesions istha tma ny lesi ons are ol dand/oras ympto ma tic. Later al osteo ch ondr al les ions are usua llysec ondary to aninj ury, sowewant to get that informa tionfr omth epa tien t. MRI can re vea lhowmuch bone ma rr owedem aispr es en tund er the lesi on. If signific an t, th en morelikel y tha n no t, th e les ion is playi ng a role. Diagn os ticinj ect ion s into th e lat eral ank le ar e of lim ited benefitbe cau seth ere wi llbe impr oveme nt wi th bot hpat hol ogi howe ver, th ere is any con ce rn of si nus tarsi syndr om e,the n a sin us tarsi inje ctio n wi th loc al ane sthesi a can ru leout tha tpot ent ialsou rc eof pa nitcom esto su rg ical repai rofthe un stab leank le,I wi ll gen eral ly do a Br ost ro m tech niq ue.
8 Us ing thestandard incis ion for lig ame nt rep air, one can acces s thelate ra l sho ulde r of the ta lus wh er e the majori ty of ost eo -ch on dral les ions are loc ated . Pl an tar flex ion of the fo otwi ll usu al ly allow you to see the cart ilagin ous defect .Debr idem ent of the cart ilag e defect an d su bch ond raldrillin gis per for med follo wed byth eligame nt repa ir. At1we ekpo st operat ive,Iwi llhav ethepat ient sta rt ank le jointac tive ran ge of mo tio n avo idin g any inver sion/e versionma ne uve rs to prote ctth eligam ent rep air. At3weeks, thepati en t wi ll sta rt wei ght bear ing in a fr act ure bo ot andret urn to sh oes at th e 6 week an nivers ary of sur gery .Ph ysi ca lthe rap yiscomme nc ed at this poin tas we e ar e 3 ana tomic are as of the foot and ank le whe rethe pe ro ne altendons will ha vepathol og y. Proxim al to theti p of the later al mal leol us is wh ere one may en co untersubl uxin g pe ro ne al te ndons or te nosy nov iti s.
9 The forme ris us ua lly assoc iated with a tr auma tic eve nt to the anklean d the latt er is us ual ly du e to an over- us e injur y. Th ere gionbe twe enth eti pofthe fibu la and the fifthmetat arsalba se is wh er e rupt ures oc cur an d mo re co mm on ly willha ve tend ino si s, a chr onic deg en erat ive stat e of ten do nwi th int er st itial tear s, and bulbous hypertrophy. Finally,pai n that is locat ed nea r th e fifth met at arsa l base isge ne ral lyatendin iti s/ent heso pa thy .MRI isuseful if one isCHAPTER314 Figure 2. Radiographof a stress fracture of thefibula. Note callus ce rned ab ou t te ndinos is. Con servati ve tre atmen ts ar era rely he lpf ul for tendinos is and will gene rall y re quir e asur gical interve nti re is a fa vor able prog nosi s with conservativetrea tment for pe roneal tendin itis that gen era lly wi ll includesom e combinationof anti -i nfla mmat ory med icat ion ,immobi liz atio n,physical th erapy, an dorthose s.
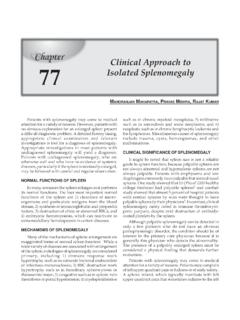
10 Awo rd ofca uti on with cort isone inj ec tions is pr udent in perone alpa tholo gy. One may consider acorti sone inje cti on into thecub ital tun ne lfo rloca lized pa in th at doe snot re sp ond toother trea tments. The inje ct ion into the cubi tal tunne l isinf eri or to the peroneusbrevis tendon. For ot her ar easal ong th eco urse of the te nd ons, un less the pati en twil lbeimmobi lize d, I will not cons ider a cort isone injectio have se en too many tendon ruptures in this ar ea aftercor tis on einj ecti on s(Figures 3an d4).SINUSTARSISYNDROMEThi sis one of those dis order sthat nobody re ally kno ws ex -act ly what it is, but it can be succes sfully trea osis of si nus tarsi syndrom eis strai ght forwa rd. Whe nth er e is pain in the sinus tars i on palpat ion and symptomsre so lve aft er injectionof local an esthet ic, one can beco nfiden t wi th the diagnos is even wi thout fur ther testin tain ly radi og raphic eva luati on is nece ssary to as sess foradva nce d ar thriti s of the subtal ar joint.