Transcription of MEDICARE DME Redetermination Request Form
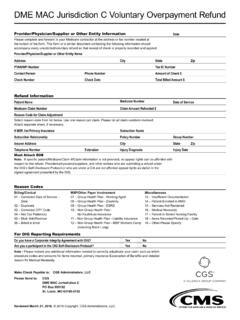
1 MEDICARE DME Redetermination Request FormJurisdiction B - CGS Administrators, LLCJ urisdiction C - CGS Administrators, LLCS upplier Information Name of Person AppealingSupplier NameAddressPhone NumberPTA NBeneficiary InformationPatient NameMedicare NumberOverpayment AppealYES If yes, who requested overpayment:Medical ReviewUPICSMRCCERTR ecovery AuditorDate of ServiceHCPCS & ModifiersCCNS uggested Documentation Check List:ABNCMNDIFP hysician s Written OrderMedical DocumentationReason for AppealIf you received your initial determination notice more than 120 days ago, include your reason for the late can now submit Redetermination forms electronically!
2 Visit the Reprocessing tab in myCGS to submit a form and see status of a Redetermination . NumbersCGS Administrators, LLC - JB Administrators, LLC - JC 1 of 1 | Revised June 3, 2020 | 2020 Copyright, CGS Administrators, LLC.