Transcription of METATARSUSADDUCTUS: …
1 INTRODUCTIONM etatarsus adductus is deformity of the foot defined as auniplanar transverse plane deformity where the metatarsalsare adducted at Lisfranc joint (1-3). The measurement ofthe metatarsus adductus angle has classically been describedas the angle between the longitudinal axis of thesecond metatarsal (representing the longitudinal axis of themetatarsus) and the longitudinal axis of the lesser tarsus. Themeasurement of the longitudinal axis of the lesser tarsus hasbeen described three ways. Classically, the longitudinalaxis of the lesser tarsus has been described as the lineperpendicular to the transverse axis of the lesser tarsus.
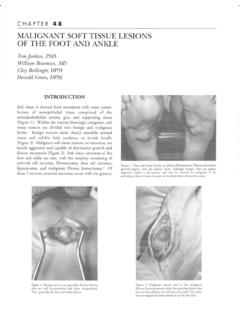
2 Twoways are described in the literature to measure the transverseaxis of the lesser tarsus. Medially, both ways use themidpoint between the line connecting the talonavicular jointand the first metatarsal cuneiform joint. Laterally, onemethod uses the lateral joint of the fourth metatarsal withthe cuboid as a reference (MAA4) (Figure 1A) (4,5).Others use the lateral joint of the fifth metatarsal with thecuboid as a reference (MAA5) (Figure 1B) (6-8). Engeldescribed the longitudinal axis of the lesser tarsus as thelongitudinal axis of the second cuneiform (Figure 1C) (9).Prior to the advent of digital radiography, MAA4 andMAA5 measurement techniques were time consuming andcumbersome for clinical practice.
3 Therefore, the simpletechnique described by Engel gained popularity. Engel sangle is much easier to draw and has also been shown byThomas (10) to be reproducible by. The MAA4 andMAA5 have both been shown to have strong intra-observer and inter-observer reliability when measuringthese angles radiographically (6,7,11-12). Although Engelconcluded that his measurement correlated well to theMAA5 technique, closer examination of the data callinto question the strength of the Pearson correlationcoefficients(r); many of the r values, although statisticallysignificant, are closer to 0 than 1 indicating poorcorrelation (9).
4 Like metatarsus adductus, digital deformity is acommon foot deformity encountered by the foot and anklesurgeon. Multiple contributing factors to the developmentof digital deformity have been suggested includingrheumatoid arthritis, plantar plate tear, secondmetatarsophalangeal joint (MPJ) stress syndrome, andimbalance between intrinsic or extrinsic musculature ofthe foot. An imbalance can occur between the intrinsic andextrinsic muscles of the foot secondary to a peripheralneuropathy such as diabetes or Charcot Marie Tooth. Inaddition, flexor stabilization, flexor substitution, andextensor substitution are all causes of imbalance betweenintrinsic and extrinsic musculature of the foot.
5 Each cause ofdigital deformity mentioned above predominantly describepathological force or imbalance in the sagittal plane. Weare not aware of any research investigating a transverse planedeformity as a possible destabilizing force across the MPJgiving rise to digital studies have suggested a larger MAA as afactor in contributing to multiple foot pathology: halluxabducto valgus (4,13,14), lateral metatarsal fractures(15,16), and hindfoot deformity (17). There have beenno studies to investigate the relationship between themetatarsus adductus angle and hammertoe metatarsal heads would move the fulcrum of theMETATARSUS ADDUCTUS:Radiographic and Pathomechanical AnalysisMichael Crawford, DPMD onald Green, DPMCHAPTER5 Figure 1A.
6 Metatarsus Adductus Angle (MAA4) using the 4thmetatarsocuboid joint as reference. Line (a) is between the most distalmedial point of the talonavicular joint and the medial point of the 1stmetatarsal cunieform joint. Line (b) is between the most lateral point ofthe calcaneo-cuboid joint and the most lateral point of the fourthmetatarsocuboid joint. (B) Metatarsus Adductus Angle (MAA5) using thelateral fifth metatarsocuboid joint as reference instead of the most lateralpoint of the fourth metatarsocuboid joint . Line (a) is between the mostdistal medial point of the talonavicular joint and the medial point of the 1stmetatarsal cunieform joint.
7 Line (b) is between the most lateral point of thecalcaneo-cuboid joint and the most lateral point of the fifth metatarsocuboidjoint. (C) Engel s Angle. Line (d) bisects the middle cuneiform. Line (e) isthe longitudinal axis of the second of the tendons across the MPJ laterally; thus causingadditional imbalance of intrinsic and extrinsic musculatureacross the aim of this study was twofold. Primarily, we wantedto investigate the relationship between metatarsus adductusangle and the presence of digital deformity to lend supportto the idea that transverse plane deformity can contribute toa primarily sagittal plane deformity of digital , we wanted to examine Engel s angle and MAA4techniques using digital radiography for reliability,reproducibility, and correlation to the traditionalmeasurement of MAA5.
8 We hypothesized that patientswith digital deformities would have significantly highermetatarsus adductus angle measurements compared topatients without digital deformity. In addition, wehypothesized that Engels angle would be reproducible butcorrelate poorly to the traditional measurement of AND METHODSP atient PopulationAnterior posterior weight-bearing radiographs from 99consecutive patients with the diagnosis of hammertoe and99 consecutive patients without hammertoe seen betweenJanuary 1, 2009 and January 31, 2013 were collectedretrospectively from the practice of the primary criteria included any patient with one or moreof the following diagnoses.
9 Rheumatoid arthritis, peripheralneuropathy, diabetes, neuromuscular disease, andCharcot-Marie-Tooth. Patients were included in thehammertoe group if they had a diagnosis of hammertoeas indicated by ICD9 code Patients were includedin the control group if they did not have any hammertoeand they did not meet any of the exclusion of the Metatarsus Adductus AngleThe metatarsus adductus angle was measured on digitalanterior posterior weight-bearing radiographs by thesecond author who was blinded to which group theradiographs belonged. Three different measurements weretaken corresponding to the three major methods ofmeasuring the metatarsus adductus angle described in theliterature (Figure 1).
10 The measurements were madeusing Tiger View imaging system angular drawing andcalculation Reliability StudyTen radiographs from each group were randomly selectedusing algorithm to generate 10 randomnumbers between 1 and 200. Those patients withcorresponding subject identification numbers wereselected to participate in the intra-rater reliability evaluator, the second author, made all threemeasurements for each radiograph at three different timesseparated by 1 week. Before each measurement session,the order of the patients was randomized so that theradiographs viewed would not be in the same order as theprevious weeks AnalysisData were analyzed using IBM SPSS professional mean (95% confidence intervals) metatarsus adductusangle measured using the three methods for each groupwere calculated.