Transcription of NATIONAL PROGRAMMES UNDER NRHM
1 69 Annual Report NATIONAL Health Programme such as the NaitonalVector Borne Diseases Control, Leprosy Eradication,TB Control, Blindness Control and Iodine DeficiencyDisorder Control PROGRAMMES have come UNDER theumbrella of NATIONAL Rural Health VECTOR BORNE DISEASECONTROL PROGRAMME (NVBDCP)The NATIONAL Vector Borne Disease Control Programme(NVBDCP) is an umbrella programme for preventionand control of vector borne diseases viz. Malaria,Japanese Encephalitis (JE), Dengue, Chikungunya, Kala-azar and Lymphatic Filariasis. Out of these six diseases,two diseases namely Kala-azar and Lymphatic Filariasishave been targeted for elimination by 2015. The Statesare responsible for implementation of programme,whereas the Directorate of NVBDCP, Delhi providestechnical assistance, policies and assistance to theStates in the form of cash & commodity, as perapproved pattern.
2 Malaria, Filaria, Japanese Encephalitis,Dengue and Chikungunya are transmitted by mosquitoeswhereas Kala-azar is transmitted by sand-flies. Thetransmission of vector borne diseases depends onprevalence of infective vectors and human-vectorcontact, which is further influenced by various factorssuch as climate, sleeping habits of human, density andbiting of vectors general strategy for prevention and control ofvector borne diseases UNDER NVBDCP is describedbelow:(i)Integrated Vector Management including IndoorResidual Spraying (IRS) in selected high risk areas,Long Lasting Insecticidal Nets (LLINs), use oflarvivorous fish, anti-larval measures in urbanChapt er 6 NATIONAL PROGRAMMES UNDER NRHM areas including bio-larvicides and minorenvironmental engineering including sourcereduction.
3 (ii)Disease Management including early casedetection with active, passive and sentinelsurveillance and complete effective treatment,strengthening of referral services, epidemicpreparedness and rapid response.(iii)Supportive Interventions including BehaviourChange Communication (BCC), Inter-sectoralConvergence, Human Resource Developmentthrough capacity building.(iv)Vaccination only against (v)Annual Mass Drugs Administration (onlyagainst Lymphatic Filariasis) )Malaria is an acute parasitic illness caused byPlasmodium falciparum or Plasmodium vivax inIndia. The main clinical presentation is with feverwith chills; however, nausea and headache can alsooccur.
4 The diagnosis is confirmed by microscopicexamination of a blood smear and RapidDiagnostic Tests. Majority of the patients recoverfrom the acute episode within a week. Malariacontinues to pose a major public health threat indifferent parts of the country, particularly due toPlasmodium falciparum severity may develop andmay cause fatality, if not treated )In India, out of 9 species of Malaria vectors, themajor vector for rural malaria is Anophelesculicifacies, found all over the country and breedsin clean ground water collections. Other importantAnopheline species namely breed in running channels, streams70 Annual Report 2013-14 The cases were contained between 2 to 3 million casesannually till 2001 afterwards the cases have furtherstarted 2011, the malaria incidence was around cases, million Pf cases and 754 deaths;while during 2012, million cases, Pf cases and519 deaths were reported.
5 About 91% of malaria casesand 99% of deaths due to malaria are reported from highdisease burden states namely North Eastern (NE) States,Andhra pradesh , Chhattisgarh, Gujarat, Jharkhand,Karnataka, Madhya pradesh , Maharashtra, Odisha,Rajasthan and West Bengal. However, other States arealso vulnerable and have local and focal 2013 (P), million cases, million Pfcases and 379 deaths have been clean water. Some of the vector species alsobreed in forest areas, mangroves, lagoons, etc,even in those with organic )In urban areas, Malaria is mainly transmitted byAnopheles stephensi which breeds in man-madewater containers in domestic and peri-domesticsituations such as tanks, wells, cisterns, which aremore or less of permanent nature and hence canmaintain density for malaria transmissionthroughout the year.
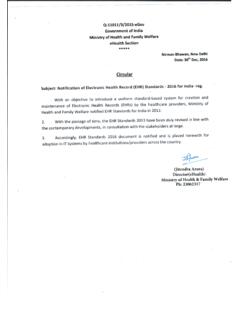
6 Increasing human activities,such as urbanization, industrialization andconstruction projects with consequent migration,deficient water and solid waste management andindiscriminate disposal of articles (tyres,containers, junk materials, cups, etc.) createmosquitogenic conditions and thus contribute tothe spread of vector borne Situation: The status of total cases, Pfcases, deaths and API from 2005 to 2013 is given in thetable and the Graph as follows. The state-wise data onmalaria cases & deaths since 2010 is at Appendix- Situation in the country during 2005-2013 Year Cases (in millions) (P) estimates of Malaria were about 75million cases and million deaths annually.
7 Theproblem was virtually eliminated in the mid-sixties butresurgence led to an annual incidence of millioncases in 1976. Modified Plan of Operation was launchedin 1977 and annual malaria incidence started in Plasmodium falciparum to Chloroquinewas observed to be very high and frequent in the studiesconducted during 2001 onwards. Therefore, ArtemisineCombination Therapy (ACT) is now being used as firstline of treatment for all Pf cases in whole of the , in North-Eastern States early signs ofresistance to currently used SP-ACT, has been noticedand so, as per the advice of Technical AdvisoryCommittee, effective combination of Artemether-Lumefantrine (ACT-AL) has been recommended for thetreatment of Pf cases in the North Eastern States.
8 Forstrengthening surveillance, Rapid Diagnostic Test (RDT)for diagnosis of malaria has also beenintroduced in high endemic areas and being scaled that about 50% of the malaria cases are dueto P vivax in the country, bivalent RDT (detecting bothPv and Pf infection) has been introduced in the countryat the field level from this year. ASHAs have beentrained in diagnosis and treatment of malaria cases andare involved in early case detection and situation in countryCases (in million)PfDeathsDeathsCases (in million)71 Annual Report 2013-14 The Government of India provides technical assistanceand logistics support including anti malaria drugs, DDT,larvicides, etc.
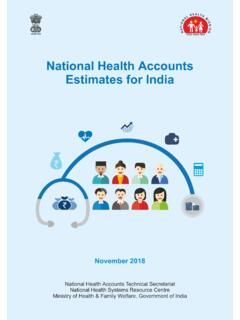
9 UNDER NVBDCP within overall umbrellaof NRHM. State Governments have to implement theprogramme and required human resource and otherlogistics are to be supported projects:Additional support for combating malaria is providedthrough external assistance in high malaria riskareas. There are two such externally funded projectswhich are currently being implemented for Fund Supported Intensified Malaria ControlProject (IMCP-II) Bank Supported Project on Malaria Control& Kala-azar areas covered UNDER these projects are as UNDER :(i)The Global Fund supported 'IntensifiedMalaria Control Project- Phase II' (IMCP-II)Global Fund Round 9 supported Intensified MalariaControl Project (IMCP-II) is being implemented sinceOctober 2010 for a period of five years in 7 NE project area covers a population of 46 million in86 districts as shown in the strategies of the project are early diagnosis andcomplete treatment, integrated vector control includingpromotion of ITN (LLINs), through intensive IEC andcapacity building & training of the health workers &community volunteers.
10 Specific inputs are provided tothese project areas in the form of manpower, RDTs,drugs and LLINs. The period for first phase is for twoyears starting from October 2010 to Sept. 2012. ThePhase-II is granted by the GFATM based on theexperience of the phase I. CARITAS India is the partnerPrincipal Recipient 2 (PR2) in the Support provided in project area is listedbelow: Human resource such as Consultants and supportstaff for project monitoring units at state and districtlevel and malaria technical supervisor andlaboratory technicians at sub-district level. Capacity building of Medical Fever Treatment Depots/Volunteersetc. Commodities such as Long-Lasting InsecticidalNets (LLINs), Rapid Diagnostic tests for quickdiagnosis of Malaria, alternate drugs based Combination Therapy and for treating severe malaria cases.