Example: dental hygienist
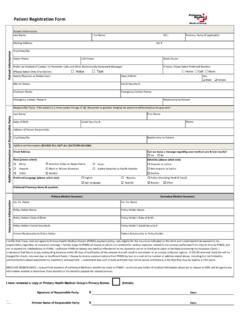
Patient Registration Form - Primary Health Medical Group
I certify that I have read and agree to Primary Health Medical Group's (PHMG) payment policy. I am eligible for the insurance indicated on this form and I understand that payment is my responsibility regardless of insurance coverage. I hereby assign to PHMG all money to which I am entitled for medical expenses related to the services performed ...
Tags:
Information
Domain:
Source:
Link to this page:
Documents from same domain
Patient Registration Form - Primary Health Medical …
www.primaryhealth.comPatient Registration Form Patient Information M.I.: Mailing Address: Apt #

PATIENT INFORMATION SHEET - Primary Health
www.primaryhealth.comPATIENT INFORMATION SHEET NAME: GENDER: DOB: DATE: ALLERGIES: List ALL MEDICATIONS you take, including over-the-counter (OTC) medications and vitamins. Include specific doses and when tak e n. I fyoud o’ tkn w, pl as cl rph mis i . PERSONAL MEDICAL HISTORY: (Please circle all that apply)

Routine Preventive Exams (Annual Physicals)
www.primaryhealth.com2. When you talk with your provider, let them know you are there for your routine preventive exam. 3. If you bring up health problems during your routine preventive exam, understand that you may have a charge related to the treatment of that problem, or the provider may ask that you schedule a separate appointment for evaluation of that problem. 4.
Related documents
Psychological health and safety in the workplace - CSA Group
www.csagroup.orgthat are directly related to mental health care. Examples include the justice system, primary health care, workplace, housing and others that impact the lives of Canadians living with a mental health problem or illness and their families. The MHCC is funded by Health Canada and has a 10-year mandate (2007-2017).
UNDERSTANDING YOUR FIDUCIARY RESPONSIBILITIES
www.dol.govcovered group health plan is an employment-based plan that provides medical care coverage, including hospitalization, sickness, prescription drugs, vision, or dental. It can provide benefits by using funds in a plan trust, purchasing insurance, or …

The State of Mental Health and Aging in America
www.cdc.govThe World Health Organization defines health as “a state of complete physical, mental, and social well-being and not merely the absence of disease or . infirmity” (1). Because mental health is essential to overall health and well-being, it must be recognized and treated in …