Transcription of Peripheral giant cell granuloma: A potentially aggressive ...
1 232 American Academy of Pediatric DentistryPediatric Dentistry 22:3, 2000 Pediatric Oral PathologyPeripheral giant cell granuloma : A potentially aggressive lesionin childrenCatherine M. Flaitz, DDS, MSDr. Flaitz is a professor, Oral and Maxillofacial Pathology and Pediatric Dentistry, Department of Stomatology, Universityof Texas at Houston Health Science Center Dental Branch, Houston, Texas. Correspond with Dr. Flaitz March 29, 2000 Revision Accepted April 3, 2000 AbstractA slowly enlarging gingival mass with a reddish-purple surfaceis observed in a school-age boy. The lesion was first noted 3 monthsago during a routine oral examination but recently it has increasedin size and interferes with eating. A periapical radiograph dem-onstrated focal loss of the alveolar crestal bone in the mandibularincisor region.
2 The diagnosis of Peripheral giant cell granuloma ,a benign reactive gingival lesion, is confirmed by histopathologicexamination. Early detection and excision of this hyperplastic nod-ule is important to minimize potential dentoalveolar complications.(Pediatr Dent 22:232-233, 2000)Solitary gingival enlargements in children are a relativelycommon finding and are usually the result of a reactiveresponse to local irritation. Although incipient lesionsmay bleed and cause minor changes in gingival contour, pro-gressive growth in some cases produces a significant tumescencethat compromises normal oral function. The purpose of thiscase report is to illustrate an example of an aggressive periph-eral giant cell granuloma (PGCG) and to discuss a reasonabledifferential diagnosis, based on the age of the patient, historyand clinical historyA 7 year old Hispanic boy is referred for evaluation of a gingi-val mass that was first observed 3 months ago during a routinedental visit.
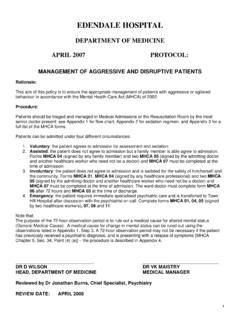
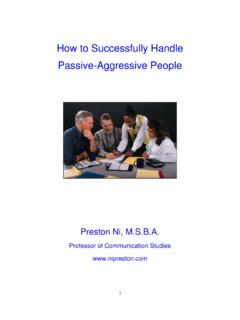
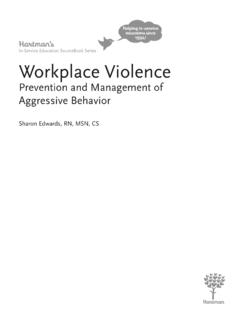
3 Recently the lesion has doubled in size and is in-terfering with normal occlusion. Clinical examination revealsa reddish-purple, sessile nodule, involving the mandibular,anterior gingiva and alveolar mucosa (Fig 1). The surface issmooth, except for focal areas of ulceration where the maxil-lary incisors are impinging on the mass. Although thenontender lesion bleeds with minimal manipulation, it doesnot blanch when palpated. The adjacent mandibular incisorsexhibit class I mobility with interproximal separation and lin-gual displacement (Fig 2). A periapical radiograph at this sitedemonstrates superficial erosion of the alveolar bone (Fig 3).No other oral or cutaneous lesions are noted in this impressionBased on the clinical presentation and history, this soft tissueenlargement is most consistent with the benign reactive lesion,PGCG or the giant cell epulis.
4 This relatively common tumor-like growth occurs exclusively on the gingiva and the alveolarmucosa and is caused by local irritation or trauma. Althoughthe peak prevalence is in the fifth and sixth decades, between20 to 33% occur within the first two decades of ,2 Themost common location for the PGCG is the incisor and ca-nine regions with a slight predilection for the , this gingival lesion presents as a rubbery, smooth-surfaced nodule or mass that is red, purple or blue in ulceration, bleeding and displacement of the teeth areFig 1. Reddish-purple nodule of the mandibular, anterior attached gingivaextends to the alveolar 2. Lingual displacement of the lateral incisor by the gingivalenlargement is Dentistry 22:3, 2000 American Academy of Pediatric Dentistry 233common findings.
5 The size of this reactive lesion varies from asmall papule to a massive enlargement; however, most lesionsare less than 2 cm in diameter. Pain is not a major complaintunless the growth is traumatized repeatedly. Radiographicevaluation of any gingival lesion, including the PGCG, is pru-dent in order to determine the extent and origin of the resorption or cupping of the alveolar bone is oftennoted on a periapical radiograph. In addition, a widened peri-odontal ligament space is associated frequently with toothmobility but may represent lesion extension around the rare instances, PGCG is an oral manifestation of hyper-parathyroidism without obvious central bony ,5 While this is an unusual initial presentation, hyperparathyroid-ism should be considered when multiple lesions are found orif repeated recurrences are documented despite adequate treat-ment.
6 A parathyroid tumor or chronic renal disease may resultin excess production of the parathyroid hormone that stimu-lates the formation of a giant cell lesion. In addition, childrenwith X-linked hypophosphatemic rickets, a condition that isassociated with subclinical hyperparathyroidism, are at in-creased risk for developing this to the large size of the lesion, an incisional biopsy, alongwith histopathologic evaluation, is recommended for the di-agnosis of this progressively enlarging gingival mass, in orderto establish a definitive diagnosis. In some cases when it is im-portant to exclude hyperparathyroidism, laboratory studiesincluding serum calcium, phosphate, alkaline phosphatase andparathyroid hormone are of this gingival lesion is surgical excision andelimination of any local contributing factors.
7 The recurrencerate is approximately 10% but multiple recurrences with even-tual loss of the adjacent teeth are a potential complication. Inthis case because of the large size of the surgical defect, a graft-ing procedure is needed to cover the exposed periosteum androots of the diagnosisGingival lesions in children that mimic the PGCG are thepyogenic granuloma , parulis and Peripheral ossifying pyogenic granuloma may be difficult to differentiate fromthe PGCG based on clinical features alone. In general the pyo-genic granuloma presents as a soft, friable nodule that bleedsfreely with minimal manipulation. Unlike the PGCG, displace-ment of teeth and resorption of alveolar bone are not erythematous nodule of the gingiva is the parulis,which is associated with an entrapped foreign body, a gingivalpocket and/or a nonvital tooth.
8 Pain and the expression of apurulent exudate with fluctuation in lesion size help to differ-entiate this inflammatory disease from the PGCG. Theperipheral ossifying fibroma is a reactive gingival growth thatshares similar clinical features as the PGCG. Although this re-active lesion is often ulcerated and inflamed, it lacks the purpleor blue discoloration that is commonly associated with thePGCG. Identification of small flecks of calcification within thetumescence on a radiograph aids in diagnosing the peripheralossifying fibroma, when present. The final consideration basedon the red or blue discoloration of the soft tissue nodule is ahemangioma. Although many hemangiomas are congenitallesions, some vascular malformations increase in size duringchildhood.
9 Brisk bleeding, increased warmth of the tissue andblanching upon palpation are characteristic of this significanceIn children, reactive oral lesions such as the PGCG can dem-onstrate a rapid growth rate and reach significant size withinseveral months of initial diagnosis. These soft tissue nodulesmay be quite aggressive and resorb bone, interfere with erup-tion of teeth and produce minor to moderate tooth are important for diagnosis to confirm that thisgiant cell lesion arises within the oral mucosa and does not rep-resent a central bony lesion with cortical perforation and softtissue extension. Early detection of the PGCG results in moreconservative surgery with less risk for tooth and bone Giansanti JS, Waldron CA. Peripheral giant cell granuloma :review of 720 cases.
10 J Oral Surg 27:787-91, Katsikeris N, Kakarantza-Angelopoulou E: Peripheral giantcell granuloma : clinicopathologic study of 224 new cases and956 reported cases. Int J Oral Maxillofac Surg 17:94-99, Pandolphi, PJ, Felefli S, Flaitz CM, Johnson JV: An aggres-sive Peripheral giant cell granuloma in a child. J Clin PediatrDent 23:353-55, Smith BR, Fowler CB: Primary hyperparathyroidism present-ing as a Peripheral giant cell granuloma . J Oral MaxillofacSurg 46:65-69, Burkes EJ, White RP: A Peripheral giant -cell granulomamanifestation of primary hyperparathyroidism: report of acase. J Am Dent Assoc 118:62-64, Stratakis CA, Mitsiades NS, Sun D, Chrousos GP, O ConnellA: Recurring oral giant cell lesion in a child with X-linkedhypophosphatemic rickets: clinical manifestation of occultparathyroidism?