Transcription of Precertification Request for Authorization of Services
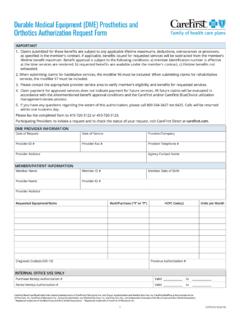
1 1 CUT9233-1E (6/18) Precertification Request for Authorization of ServicesINSTRUCTIONSFor fax requests onlyPlease complete all fields for a timely response to avoid a delay of Authorization . In most cases, you should receive a response via fax or telephone within two business days. Please fax only the Authorization Request form to 410-781-7661. If requesting an Authorization for a carefirst employee, fax the Request to 410-505-2840. Please submit this completed form only at this time. Additional clinical information will be requested if from: Doctor s office Hospital Participating Providers: to initiate a Request and to check the status of your Request , visit carefirst Direct at Please fax Authorization Request to #Fax #Participating Provider #, NPI or Tax ID# (under which you will bill claims)Patient s NameDate of BirthPatient s Identification #Group #AddressTelephone #CityStateZip CodeDate(s) of Service or Admit Date(s)Place of Service (check one) Inpatient Facility Outpatient Facility Emergency Room Admit Physician s OfficeAdmitting/Treating Physician s NameTelephone #Physician s AddressDiagnosis Code(s) (ICD-10)Procedure Code(s) (CPT-4)Hospital/FacilityTelephone #Hospital/Facility AddressHospital/Facility Telephone #Referral # (if applicable)
2 Referral Issue DateAUTHORIZATION NUMBER (FOR INTERNAL OFFICE USE ONLY)Associate NameCompleted byDateTimeCommentsCareFirst BlueCross BlueShield is the shared business name of carefirst of Maryland, Inc. and Group Hospitalization and Medical Services , Inc. carefirst MedPlus is the business name of First Care, Inc. carefirst of Maryland, Inc., Group Hospitalization and Medical Services , Inc. and First Care, Inc., are independent licensees of the Blue Cross and Blue Shield Association. Registered trademark of the Blue Cross and Blue Shield Association. Registered trademark of carefirst of Maryland, of Nondiscrimination and Availability of Language Assistance ServicesCareFirst BlueCross BlueShield, carefirst BlueChoice, Inc. and all of their corporate affiliates ( carefirst ) comply with applicable federal civil rights laws and do not discriminate on the basis of race, color, national origin, age, disability or sex.
3 carefirst does not exclude people or treat them differently because of race, color, national origin, age, disability or : Provides free aid and Services to people with disabilities to communicate effectively with us, such as:Qualified sign language interpretersWritten information in other formats (large print, audio, accessible electronic formats, other formats) Provides free language Services to people whose primary language is not English, such as:Qualified interpretersInformation written in other languagesIf you need these Services , please call you believe carefirst has failed to provide these Services , or discriminated in another way, on the basis of race, color, national origin, age, disability or sex, you can file a grievance with our carefirst Civil Rights coordinator by mail, fax or email.
4 If you need help filing a grievance, our carefirst Civil Rights coordinator is available to help you. To file a grievance regarding a violation of federal civil rights, please contact the Civil Rights coordinator as indicated below. Please do not send payments, claims issues, or other documentation to this Rights coordinator , Corporate Office of Civil RightsMailing Address Box 8894 Baltimore, Maryland 21224 Email Address Number 410-528-7820 Fax Number 410-505-2011 You can also file a civil rights complaint with the Department of Health and Human Services , Office for Civil Rights electronically through the Office for Civil Rights Complaint portal, available at or by mail or phone Department of Health and Human Services 200 Independence Avenue, SW Room 509F, HHH Building Washington, 20201 800-368-1019, 800-537-7697 (TDD)Complaint forms are available at BlueCross BlueShield is the shared business name of carefirst of Maryland, Inc.
5 And Group Hospitalization and Medical Services , Inc. carefirst of Maryland, Inc., Group Hospitalization and Medical Services , Inc., carefirst BlueChoice, Inc., The Dental Network and First Care, Inc. are independent licensees of the Blue Cross and Blue Shield Association. In the District of Columbia and Maryland, carefirst MedPlus is the business name of First Care, Inc. In Virginia, carefirst MedPlus is the business name of First Care, Inc. of Maryland (used in VA by: First Care, Inc.). Registered trademark of the Blue Cross and Blue Shield Association. Registered trademark of carefirst of Maryland, (12/17) Foreign Language Assistance Attention (English): This notice contains information about your insurance coverage. It may contain key dates and you may need to take action by certain deadlines.
6 You have the right to get this information and assistance in your language at no cost. Members should call the phone number on the back of their member identification card. All others may call 855-258-6518 and wait through the dialogue until prompted to push 0. When an agent answers, state the language you need and you will be connected to an interpreter. (Amharic) - 855-258-6518 0 d Yor b (Yoruba) t t l ko: k y s y n w f n n pa i ad j t f r.
7 Le n w n d t p t o s le n l ti gb gb s n w n j gb d ke kan. O ni t l ti gba w f n y ti r nl w n d r l f . w n m - gb gb d pe n mb f n t w l y n k d d nim w n. w n m r n le pe 855-258-6518 k o s d r n pas j r r t t a fi s f n l ti t 0. N gb t a oj kan b d h n, s d t o f a s so p m gbuf kan. Ti ng Vi t (Vietnamese) Ch : Th ng b o n y ch a th ng tin v ph m vi b o hi m c a qu v . Th ng b o c th ch a nh ng ng y quan tr ng v qu v c n h nh ng tr c m t s th i h n nh t nh. Qu v c quy n nh n c th ng tin n y v h tr b ng ng n ng c a qu v ho n to n mi n ph . C c th nh vi n n n g i s i n tho i m t sau c a th nh n d ng. T t c nh ng ng i kh c c th g i s 855-258-6518 v ch h t cu c i tho i cho n khi c nh c nh n ph m 0.
8 Khi m t t ng i vi n tr l i, h y n u r ng n ng qu v c n v qu v s c k t n i v i m t th ng d ch vi n. Tagalog (Tagalog) Atensyon: Ang abisong ito ay naglalaman ng impormasyon tungkol sa nasasaklawan ng iyong insurance. Maaari itong maglaman ng mga pinakamahalagang petsa at maaaring kailangan mong gumawa ng aksyon ayon sa ilang deadline. May karapatan ka na makuha ang impormasyong ito at tulong sa iyong sariling wika nang walang gastos. Dapat tawagan ng mga Miyembro ang numero ng telepono na nasa likuran ng kanilang identification card. Ang lahat ng iba ay maaaring tumawag sa 855-258-6518 at maghintay hanggang sa dulo ng diyalogo hanggang sa diktahan na pindutin ang 0. Kapag sumagot ang ahente, sabihin ang wika na kailangan mo at ikokonekta ka sa isang interpreter.
9 Espa ol (Spanish) Atenci n: Este aviso contiene informaci n sobre su cobertura de seguro. Es posible que incluya fechas clave y que usted tenga que realizar alguna acci n antes de ciertas fechas l mite. Usted tiene derecho a obtener esta informaci n y asistencia en su idioma sin ning n costo. Los asegurados deben llamar al n mero de tel fono que se encuentra al reverso de su tarjeta de identificaci n. Todos los dem s pueden llamar al 855-258-6518 y esperar la grabaci n hasta que se les indique que deben presionar 0. Cuando un agente de seguros responda, indique el idioma que necesita y se le comunicar con un int rprete. Русский (Russian) Внимание! Настоящее уведомление содержит информацию о вашем страховом обеспечении. В нем могут указываться важные даты, и от вас может потребоваться выполнить некоторые действия до определенного срока.
10 Вы имеете право бесплатно получить настоящие сведения и сопутствующую помощь на удобном вам языке. Участникам следует обращаться по номеру телефона, указанному на тыльной стороне идентификационной карты. Все прочие абоненты могут звонить по номе ру 855-258-6518 и ожидать, пока в голосовом меню не будет предложено нажать цифру 0 . При ответе агента укажите желаемый язык общения, и вас свяжут с переводчиком. (Hindi) : - 855-258-6518 0 , s -w (Bassa) To u u Ca o!