Transcription of PRESCRIPTION DRUG MEDICATION REQUEST FORM FAX TO 1 …
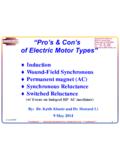
1 Medical Rationale / Reason for Drug Therapy / Treatment PlanAlternatives Tried / Used By Patient (if applicable)CLINICAL / MEDICATION INFORMATIONPHYSICIAN INFORMATION(needed for mailing notification - please print legibly)FOR INTERNAL REVIEWPATIENT INFORMATIONPRESCRIPTION DRUGMEDICATION REQUEST FORMFAX TO 1-412-544-7546 Please use separate form for each drug. Print, type or WRITE LEGIBLY and complete the form in reverse side for additional detailsOnce a clinical decision has been made, a decision letter will be mailed to the patient and other helpful information, please visit the Highmark Web site view the formulary on-line, please visit our Web site at (R10-03) 22645 Subscriber ID NumberGroup NumberPatient NameDate of BirthPatient AddressCityStateZip CodeDrug NameStrength or DoseRequested Quantity per MonthDiagnosisDrug NameStrengthDocumentation of Failure of TherapyDrug NameStrengthDocumentation of Failure of TherapyDrug NameStrengthDocumentation of Failure of TherapyPhysician NamePhoneFaxPhysician AddressCityStateZip CodeSuite / BuildingPhysician SignatureDate Approved Denied Not Applicable Benefit DenialReason CodeReceived DateDecision DateReviewer1.
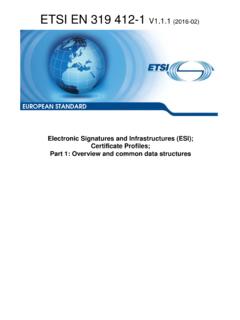
2 Submit a separate form for each Complete ALLinformation on the :The prescribing physician (PCP or Specialist) should, in most cases, complete the Please provide the physician address as it is required for physician Fax the completedform to 1-412-544-7546Or mail the form to:Medical & Pharmacy Box 279; Pittsburgh, PA 15230 Clinical Management ProceduresIn general, when requesting coverage for a MEDICATION , the following information in the bullet points below isrequired:Non-Formulary Most products: documentation of a trial of at least two formulary products Beta-blockers, calcium channel blockers, or analgesics: documentation of a trial of at least three formularyproductsPrior AuthorizationFor the following drugs and/or therapeutic categories, the diagnosis, applicable lab data, and involvement ofspecialists are required, plus additional information as specified: Anti-rheumatic drugs (Enbrel, Humira, Kineret) Forteo: at least two other osteoporotic therapies and risk for fractures ( , T-score) Growth Hormone: bone age, growth chart, and stim tests Smoking Cessation: treatment plan also required Wellbutrin: not covered for smoking cessation therapyMiscellaneous Items.
3 Contraceptives, Fertility agents, Gleevec, Interferons, Iressa, Provigil, Retin-A, TracleerManaged PRESCRIPTION Drug Coverage (MRxC)For the following drugs and/or therapeutic categories, the diagnosis, quantity requested, and alternativestriedare required. Migraine: preventative medications, if applicable Onychomycosis (Lamisil and Sporanox) Leukotriene Modifiers (Singulair, Accolate, and Zyflo) Pain Management: treatment plan also required COX-II Inhibitors and Anti-Secretory Agents (H2antagonists and proton pump inhibitors): please callour claims processor at view the formulary on-line, please visit our Web site at for Completing the Form