Transcription of Prescription Drug Prior Authorizathion Request Form - Aetna
1 Fax this form to: 1-877-269-9916. Aetna Specialty Pharmacy phone: 1-855-240-0535. OR. Submit your Request online at: Prescription drug Prior authorization Request FORM. CONTAINS CONFIDENTIAL PATIENT INFORMATION. For FASTEST service, call 1-855-240-0535, Monday-Friday, 8 to 6 Central Time Urgent1 Non-Urgent Requested drug Name: Is this drug intended to treat opioid dependence? Yes No If Yes, is this a first Request within a 12-month period for Prior authorization for this drug ? *If Yes, Prior authorization is not required for a 5-day supply of any FDA approved drug for the treatment of opioid dependence and there is no need to complete this form. Yes* No *If No, as of January 1, 2020, a Prior authorization is not required for Prescription medications on the carrier's formulary and there is no need to complete this form.
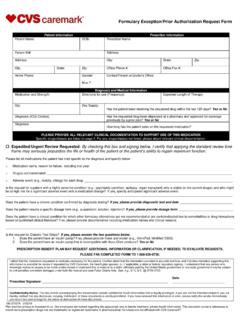
2 Patient Information: Prescribing Provider Information: Patient Name: Prescriber Name: Member/Subscriber Number: Prescriber Fax: Policy/Group Number: Prescriber Phone: Patient Date of Birth (MM/DD/YYYY): Prescriber Pager: Patient Address: Prescriber Address: Patient Phone: Prescriber Office Contact: Patient Email Address: Prescriber NPI: Prescriber DEA: Prescription Date: Prescriber Tax ID: Specialty/Facility Name (If Applicable): Prescriber Email Address: Prior authorization Request for drug Benefit: New Request Reauthorization Patient Diagnosis and ICD Diagnostic Codes(s): drug (s) Requested (with J-Code, if applicable): Strength/Route/Frequency: Unit/Volume of Named drug (s): Start Date and Length of Therapy: Location of Treatment ( provider office, facility, home health, etc.)
3 Including name, Type 2 NPI (if applicable), address and tax ID: Clinical Criteria for Approval, Including other Pertinent Information to Support the Request , other Medications Tried, Their Name(s), Duration, and Patient Response: Any additional information we should consider (please attach all supporting documents). For use in clinical trial? (if yes, provide trial name and registration number): drug Name (Brand Name and Scientific Name)/Strength: Dose: Route: Frequency: Quantity: Number of Refills: Product will be delivered to: Patient's Home Physician Office Other: Prescriber or Authorized Signature: Date: Dispensing Pharmacy Name and Phone Number: Approved Denied If denied, provide reason for denial, and include other potential alternative medications, if applicable, that are found in the formulary of the carrier.
4 1. A Request for Prior authorization that if determined in the time allowed for non-urgent requests could seriously jeopardize the life or health of the covered person or the ability of the covered person to regain maximum function, could subject the person to severe pain that cannot be adequately managed without the drug benefit contained in the Prior authorization Request or is a Prior authorization Request for medication assisted treatment for substance abuse disorders. GR-69025-1 CO (8-20). Aetna complies with applicable Federal civil rights laws and does not unlawfully discriminate, exclude or treat people differently based on their race, color, national origin, sex, age, or disability. We provide free aids/services to people with disabilities and to people who need language assistance.
5 If you need a qualified interpreter, written information in other formats, translation or other services, call the number on your ID card. If you believe we have failed to provide these services or otherwise discriminated based on a protected class noted above, you can also file a grievance with the Civil Rights Coordinator by contacting: Civil Rights Coordinator, Box 14462, Lexington, KY 40512 (CA HMO customers: PO Box 24030 Fresno, CA 93779), 1-800-648-7817, TTY: 711, Fax: 859-425-3379 (CA HMO customers: 860-262-7705), You can also file a civil rights complaint with the Department of Health and Human Services, Office for Civil Rights Complaint Portal, available at , or at: Department of Health and Human Services, 200 Independence Avenue SW., Room 509F, HHH Building, Washington, DC 20201, or at 1-800-368-1019, 800-537-7697 (TDD).
6 Aetna is the brand name used for products and services provided by one or more of the Aetna group of subsidiary companies. GR-69025-1 CO (8-20). TTY:711. English To access language services at no cost to you, call the number on your ID card. P r sh rbime p rkthimi falas p r ju, telefononi n numrin q gjendet n kart n tuaj t . Albanian identitetit. Amharic . Arabic .. Armenian .. Bantu-Kirundi Kugira uronke serivisi z'indimi ata kiguzi, hamagara inomero iri ku karangamuntu kawe Bengali Burmese Per accedir a serveis ling stics sense cap cost per a vost , telefoni al n mero indicat a la seva Catalan targeta d'identificaci . Aron maakses ang mga serbisyo sa lengguwahe nga wala kay bayran, tawagi ang numero nga Cebuano anaa sa imong kard sa ID. Para un hago' i setbision lenggu hi ni dib tde para h gu, gang i numiru gi iyo-mu kard Chamorro aidentifikasion.
7 , . Cherokee ID . Chinese . Traditional Anumpa tosholi i toksvli ya peh pilla ho ish i payahinla kvt chi holisso kallo iskitini holhtena Choctaw takanli ma i payah Ren omw kopwe angei aninisin eman chon awewei (ese kam ), kopwe k ri ewe nampa mei Chuukese mak won noum ena katen ID. Cushitic- Tajaajiiloota afaanii gatii bilisaa ati argaachuuf,lakkoofsa fuula waraaqaa eenyummaa (ID) kee Oromo irraa jiruun bilbili. Dutch Voor gratis taaldiensten, bel het nummer op uw ziekteverzekeringskaart. Pour acc der gratuitement aux services linguistiques, veuillez composer le num ro indiqu sur French votre carte d'assurance sant . French Creole Pou ou jwenn s vis gratis nan lang ou, rele nimewo telef n ki sou kat idantifikasyon asirans (Haitian) sante ou. Um auf den f r Sie kostenlosen Sprachservice auf Deutsch zuzugreifen, rufen Sie die Nummer German auf Ihrer ID-Karte an.
8 , . Greek . Gujarati No ka wala au ana me ka lawelawe lelo e kahea aku i ka helu kelepona ma k u k leka ID. K ki Hawaiian ole ia k ia k kua nei. Hindi Yuav kom tau kev pab txhais lus tsis muaj nqi them rau koj, hu tus naj npawb ntawm koj daim Hmong npav ID. GR-69025-1 CO (8-20). Igbo Inweta enyemaka as s na akwughi gw ob la, kp n mba n na kaadi njirimara g . Tapno maakses dagiti serbisio ti pagsasao nga awanan ti bayadna, awagan ti numero nga adda Ilocano ayan ti ID kardmo. Untuk mengakses layanan bahasa tanpa dikenakan biaya, silakan hubungi nomor telepon di Indonesian kartu asuransi Anda. Per accedere ai servizi linguistici senza alcun costo per lei, chiami il numero sulla tessera Italian identificativa. Japanese ID . Karen Korean ID . I nyuu kosna mahola ni language services ngui nsaa wogui wo, sebel i nsinga i ye ntilga i kat yong Kru-Bassa matibla Kurdish Lao.
9 , .. Marathi an b k jipan k n kajin ilo an ejje k w ean nan kwe, kw n kallok n ba eo ilo kaat in ID eo Marshallese a . Micronesian- Pwehn alehdi sawas en lokaia kan ni sohte pweipwei, koahlih nempe nan amhw doaropwe en ID. Ponapean Mon-Khmer, Cambodian Navajo Nepali de thokic ke c n w u k r keek t n y n. Ke y n c l ran ye k c ku ny n . T k r y n ran de w r Nilotic-Dinka namba de abac t n ID kard du n de t t de nyin de panakim k u.. Norwegian For tilgang til kostnadsfri spr ktjenester, ring nummeret p ID-kortet ditt. Pennsylvanian- Um Schprooch Services zu griege mitaus Koscht, ruff die Nummer uff dei ID Kaart. Dutch Persian Farsi .. Aby uzyska dost p do bezp atnych us ug j zykowych, nale y zadzwoni pod numer podany na Polish karcie identyfikacyjnej.
10 Para aceder aos servi os lingu sticos gratuitamente, ligue para o n mero indicado no seu cart o Portuguese de identifica o. Punjabi Romanian Pentru a accesa gratuit serviciile de limb , apela i num rul de pe cardul de membru. Для того чтобы бесплатно получить помощь переводчика, позвоните по телефону, Russian приведенному на вашей идентификационной карте. M le mauaina o 'au'aunaga tau gagana e aunoa ma se totogi, vala'au le numera i luga o lau Samoan pepa ID. Serbo-Croatian Za besplatne prevodila ke usluge pozovite broj naveden na Va oj identifikacionoj kartici. GR-69025-1 CO (8-20). Para acceder a los servicios ling sticos sin costo alguno, llame al n mero que figura en su tarjeta Spanish de identificaci n. Sudanic Hee a a naasta nder ekkitol jaangirde woldeji walla yo ugo, ewnu lamba je on windi ha do Fulfulde erowol maa a.