Example: bachelor of science
Prescription Drug Prior Authorizathion Request Form - Aetna
Fax this form to: 1-877-269-9916 OR Submit your request online at: www.availity.com CALIFORNIA PRESCRIPTION DRUG PRIOR AUTHORIZATION OR STEP THERAPY EXCEPTION REQUEST FORM Patient Name: ID#: Instructions: Please fill out all applicable sections on both pages completely and legibly.
Tags:
Information
Domain:
Source:
Link to this page:
Documents from same domain

How to use electronic referrals - Aetna
www.aetna.comSpecialty family Aetna specialties Taxonomy code GASTROENTEROLOGY Colon and rectal surgery Gastroenterology Gastroenterology (pediatric) Hepatology Proctology 207RG0100X GENERAL PRACTICE Adolescent medicine Developmental medicine

PLAN DESIGN AND BENEFITS PROVIDED BY …
www.aetna.comCustom Medicare HMO Open Access Plan State of New Jersey PLAN DESIGN AND BENEFITS Aetna Medicare SM Plan (HMO) PROVIDED BY AETNA HEALTH INC Arizona, California, Connecticut, Delaware, District of Columbia, Florida, Georgia, Illinois, Maryland, Maine, New

You don’t join us, we join youSM - Aetna
www.aetna.comOur Code of Conduct is grounded in and reflects the principles at the heart of The Aetna Way. The Code guides our compliance with the rules and regulations that govern our business throughout the world.

Ptosis Surgery Precertification Information …
www.aetna.comPCFX . Ptosis Surgery Precertification Information Request Form . About this form . You can’t use this form to initiate a precertification request.

Find out how members can save on lab costs - Aetna
www.aetna.com• Accu Reference Medical Laboratory, LLC • Advanced Clinical Laboratory Solutions, Inc. • Alere Toxicology • Ameritox • ARL/Labsouth, Inc.

Coverage of Experimental and Investigational …
www.aetna.comCoverage of Experimental and Investigational Procedures Policy Aetna covers experimental or investigational technologies (i.e., …

Great Savings on Hearing Aids - Aetna
www.aetna.comGreat Savings on Hearing Aids! Hearing loss is the third most prevalent medical condition among Americans over age 65 after arthritis and hypertension.

Volume 10, Issue 1 Aetna OfficeLink Updates
www.aetna.comQuality health plans & benefits Healthier living Financial well-being Intelligent solutions March 2013 • Volume 10, Issue 1 Mid-America Region

Aetna OfficeLink Updates - All regions September …
www.aetna.comSeptember 2017 Aetna OfficeLink Updates™ All regions Inside this issue Updates to our precertification list 2 Clinical payment, coding and policy updates 3 – 4

A quick reference guide for health care …
www.aetna.comQuality health plans & benefits Healthier living Financial well-being Intelligent solutions. A quick reference guide for health care professionals
Related documents
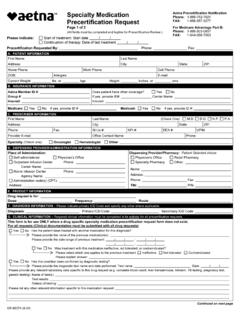
Specialty Medication Precertification Request - Aetna
www.aetna.comPrecertification Request Aetna Precertification Notification Phone: 1-866-752-7021 FAX: 1-888-267-3277 For Medicare Advantage Part B: Phone: 1-866-503-0857 FAX: 1-844-268-7263 (All fields must be completed and legible for Precertification Review.) Please indicate: Start of treatment: Start date. Continuation of therapy: Date of last treatment