Transcription of Prescription Drug Reimbursement Claim Form - …
1 Prescription drug Reimbursement Claim form Express Scripts is an independent company that provides pharmacy services for Blue Cross Blue Shield of Michigan. Instructions: Please read carefully or claims may be time and money. In the future, present your Blue Cross Blue Shield of Michigan ID card at a participating pharmacy and ask them to submit your Prescription Claim electronically. We have over 50,000 pharmacies in our network. Submission Requirements Claims must be submitted within one year of the date of service. Claims over one year will not bereimbursed. Pharmacy receipts are required for each register receipts are not you don t have a pharmacy receipt, ask your pharmacy to provide one to you.
2 The following information is required to process your to your pharmacy receipt or contact your pharmacy for missing information. Patient name and date of birth Prescribing physician name and NPI number Pharmacy name, address and telephone number Date of service Prescription number Name and strength of Prescription dispensed National drug Code (also referred to as NDC) Quantity Day supply Amount paidGeneral Instructions 1. Complete this Claim form if you paid full price for a Prescription and the pharmacy did not submit aclaim to Blue Cross or if you are submitting for Coordination of Complete a separate Claim form for each patient and for each prescribing physician and/or a pharmacy receipt for each Prescription submitted for Read the acknowledgement carefully and sign and date the Claim form .
3 A signature is required toprocess your Return the completed Claim form and pharmacy receipt(s) to:Express ScriptsATTN: Commercial Box 14711 Lexington, KY 40512-4711Or you may fax your Claim form and pharmacy receipt(s) to: do not combine claims for different patients in the same fax drug Reimbursement Claim form Express Scripts is an independent company that provides pharmacy services for Blue Cross Blue Shield of Michigan. Foreign PrescriptionsYou may qualify for a vacation supply of your Prescription prior to traveling outside of the United States. For more information, call the Customer Service number located on the back of your Blue Cross Blue Shield of Michigan ID Prescription Requirements Medication purchased outside of the United States must have an FDA approved American Equivalentto be considered for Reimbursement .
4 Medication purchased and shipped to you from a pharmacy outside of the United States will not bereimbursed. Claims must be submitted within one year of the date of service. Claims over one year will not bereimbursed. Pharmacy receipts are required for each Prescription . The following information is required to process a foreign Claim . Patient name and date of birth Pharmacy name, address and telephone number Date of service Name and strength of Prescription dispensed Quantity Day supply Amount paid Country Currency used Coordination of Benefits InstructionsIf Blue Cross Blue Shield of Michigan is your secondary Prescription drug plan, complete the following steps for consideration of payment.
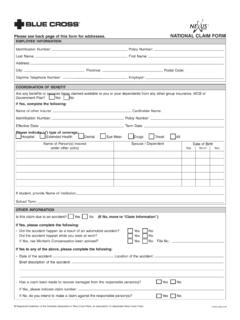
5 1. The Claim must first be submitted to the primary Prescription drug plan for consideration of Once the primary plan has processed the Claim , complete this Claim Provide your secondary Blue Cross group number and enrollee ID in the Cardholder Check the box for Another health plan paid a portion in the Coordination of Benefits Attach the Explanation of Benefits (EOB) statement from the primary plan. The EOB statement shouldclearly indicate the cost of the Prescription and what was paid by the primary plan. If the primary plandidn t provide an EOB statement, attach the pharmacy receipt. An EOB or pharmacy receipt isrequired to process your $GGUHVV&LW\6 WDWH =,3/DVW1 DPH RI 3 KDUPDF\6 WUHHW $GGUHVV&LW\6 WDWH =,3 Express Scripts is an independent company that provides pharmacy services for Blue Cross Blue Shield of Michigan.
6 @@@@@@@@@@@@@@@@@@@@@@@@@@@@@@ 'DWH@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@@ @@@@@@@@@@@@@@@@@@@@@@@@@@@ (QUROOHH RU 3 DWLHQW 6 LJQDWXUH 5(48,5(' &DUGKROGHU ,QIRUPDWLRQ UHIHU WR \RXU %OXH &URVV ,' FDUG %&%60$1 % &KHFN \RXU 5[*US*URXS 1 XPEHU3 UHVFULSWLRQ 'UXJ 5 HLPEXUVHPHQW &ODLP )RUP&RPSOHWH WKH IURQW DQG EDFN RI WKH FODLP IRUP DQG LQFOXGH SKDUPDF\ UHFHLSWV &ODLPV PD\ EH GHQLHG LI LQFRPSOHWH $OOHUJ\ 6 HUXP&RPSRXQG 3 UHVFULSWLRQ$VN \RXU SKDUPDFLVW WR FRPSOHWH WKH &RPSRXQG 3 UHVFULSWLRQ VHFWLRQ RQ WKH EDFN RI WKH FODLP IRUP )RUHLJQ 3 UHVFULSWLRQ 0 HGLFDWLRQ SXUFKDVHG RXWVLGH RI WKH 8 QLWHG 6 WDWHV PXVW KDYH DQ )'$ DSSURYHG $PHULFDQ (TXLYDOHQW WR EH FRQVLGHUHG IRU UHLPEXUVHPHQW 3 OHDVH LQGLFDWH &RXQWU\ BBBBBBBBBBBBBBBBBBBBBBBB&XUUHQF\ XVHG BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB BBBBBBBBBB3 DWLHQW ,QIRUPDWLRQ $QRWKHU KHDOWK SODQ SDLG D SRUWLRQ UHIHU WR &RRUGLQDWLRQ RI %HQHILWV ,QVWUXFWLRQV 'LVFRXQW FDUG RU FRXSRQ ZDV XVHG $FNQRZOHGJPHQW3 DWLHQW 1 DPH )]
7 LUVW BBBBBBBBBBBBBBBB3 KDUPDF\ UHFHLSWV DUH UHTXLUHG IRU DOO FODLPV 6HH EDFN RI WKH FODLP IRUP IRU GHWDLOV &KHFN WKH DSSURSULDWH ER[ LI \RXU FODLP LV IRU $Q\ SHUVRQ ZKR NQRZLQJO\ DQG ZLWK LQWHQW WR GHIUDXG LQMXUH RU GHFHLYH DQ\ LQVXUDQFH FRPSDQ\ VXEPLWV D FODLP RU DSSOLFDWLRQ FRQWDLQLQJ DQ\ PDWHULDOO\ IDOVH GHFHSWLYH LQFRPSOHWH RU PLVOHDGLQJ LQIRUPDWLRQ SHUWDLQLQJ WR VXFK FODLP PD\ EH FRPPLWWLQJ D IUDXGXOHQW LQVXUDQFH DFW ZKLFK LV D FULPH DQG PD\ VXEMHFW VXFK SHUVRQ WR FULPLQDO RU FLYLO SHQDOWLHV LQFOXGLQJ ILQHV DQG RU LPSULVRQPHQW RU GHQLDO RI EHQHILWV , FHUWLI\ WKDW WKH PHGLFDWLRQ V GHVFULEHG ZDV UHFHLYHG IRU XVH E\ WKH SDWLHQW OLVWHG DERYH DQG WKDW , RU WKH SDWLHQW LI QRW P\VHOI DP HOLJLEOH IRU SUHVFULSWLRQ GUXJ EHQHILWV , FHUWLI\ WKDW WKH PHGLFDWLRQ V GHVFULEHG ZHUH QRW IRU DQ RQ WKH MRE LQMXU\ %\ FRPSOHWLQJ WKLV IRUP , UHFRJQL]H WKDW UHLPEXUVHPHQW ZLOO EH SDLG GLUHFWO\ WR PH DQG WKDW DVVLJQPHQW RI WKHVH EHQHILWV WR D SKDUPDF\ RU DQ\ RWKHU SDUW\ LV YRLG BBBBBBBBBBBBBBBB(QUROOHH ,' ODVW QLQH QXPEHUV RQO\ ([DPSOH $%& BBBBBBBBBB(QUROOHH 1 DPH )))]
8 LUVW&RRUGLQDWLRQ RI %HQHILWV,QGLFDWH WKH JURXS QXPEHU DQG HQUROOHH ,' RI \RXU VHFRQGDU\ FRYHUDJH &KHFN WKH DSSURSULDWH ER[ EHORZ 7 HOHSKRQH LQFOXGH DUHD FRGH 3 KDUPDF\ ,QIRUPDWLRQBBBBBBBBBBBBBBBBBBBBBBBBBBBBB BBBBBBBBBBBBBBBBBBB3 DWLHQW 'DWH RI %LUWK 00 '' <<<< BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB BBBBBBBB3 UHVFULELQJ 3K\VLFLDQ ,QIRUPDWLRQ 1 DPH RI 3 UHVFULELQJ 3K\VLFLDQBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB BBBBBBBBBBBBBBBBB'D\WLPH 7 HOHSKRQH LQFOXGLQJ DUHD FRGH BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB BBBBBBBB,V WKLV DQ RQ VLWH QXUVLQJ KRPH SKDUPDF\"<HV 1R13, 1 DWLRQDO 3 URYLGHU ,GHQWLILHU ML6760D,QFOXGH D GHWDLOHG SKDUPDF\ UHFHLSW IRU HDFK SUHVFULSWLRQ ,I \RX GRn'W KDYH D SKDUPDF\ UHFHLSW DVN \RXU SKDUPDF\ WR SURYLGH RQH to you &RPSOHWH WKH FODLP LQIRUPDWLRQ EHORZ $OO ILHOGV DUH UHTXLUHG WR SURFHVV \RXU FODLP 5 HIHU WR \RXU SKDUPDF\ UHFHLSW RU FRQWDFW \RXU SKDUPDF\ IRU PLVVLQJ LQIRUPDWLRQ &203281' 35(6&5,37,21 21/<3 UHVFULSWLRQ 4 XDQWLW\ 'D\ 6 XSSO\'DWH RI 6 HUYLFH,QJUHGLHQW 1'& 1 XPEHU 0 HWULF 4 XDQWLW\ ,QJUHGLHQW &RVWP ennsylvania.)]
9 Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of Claim containing anymaterially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects such person to criminal and civil penalties. California: For your protection, California law requires the following to appear on this form : Any person who knowingly presents false or fraudulent Claim for the payment of a loss is JXLOW\ RI D FULPH DQG PD\ EH VXEMHFW WR ILQHV DQG FRQILQHPHQW LQ VWDWH SULVRQ 123456 5 HWXUQ WKH FRPSOHWHG FODLP IRUP DQG UHFHLSW V WR ([SUHVV 6 FULSWV $771 &RPPHUFLDO &ODLPV 3 2 %R[ /H[LQJWRQ.)]]]
10 < v6 XEPLW RQH FODLP IRUP SHUFRPSRXQG SUHVFULSWLRQ v/LVW D YDOLG GLJLW 1'&QXPEHU IRU HDFK LQJUHGLHQW LQWKH FRPSRXQG v,QGLFDWH WKH PHWULF TXDQWLW\ QXPEHU RI WDEOHWV JUDPV PLOOLOLWHUV HWF IRU HDFK 1'& v,QGLFDWH WKH LQJUHGLHQW FRVWIRU HDFK 1'& v,QGLFDWH WKH DPRXQW SDLG IRUWKH FRPSRXQG SUHVFULSWLRQ v,QFOXGH D GHWDLOHG SKDUPDF\UHFHLSW ZLWK WKLV FODLP IRUP BBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBBB$PRXQW 3 DLG2U \RX PD\ ID[ \RXU FODLP IRUP DQG UHFHLSW V WR 3 OHDVH GR QRW FRPELQH FODLPV IRU GLIIHUHQW SDWLHQWV LQ WKH VDPH ID[ VXEPLVVLRQ v&DVK UHJLVWHU UHFHLSWV DUH QRW DFFHSWHG v&ODLPV PXVW EH VXEPLWWHG ZLWKLQ RQH \HDU RI WKH GDWH RI VHUYLFH 1 DWLRQDO 'UXJ &RGH GLJLW 1'& ,I VXEPLWWLQJ D IRUHLJQ SUHVFULSWLRQ OHDYH WKLV ILHOG EODQN 3 UHVFULSWLRQ 1 DPH 6 WUHQJWK3 UHVFULSWLRQ1 XPEHU'DWH RI 6 HUYLFH00 '' <<<<4 XDQWLW\'D\ 6 XSSO\ 'D\ 'D\27+(5 VSHFLI\ $PRXQW 3 DLG,I VXEPLWWLQJ D IRUHLJQ SUHVFULSWLRQ OHDYH WKLV ILHOG EODQN 3 KDUPDF\ 5 HFHLSWV DUH 5(48.))]]