Transcription of Recurring Premium Reimbursement Form - Via Benefits
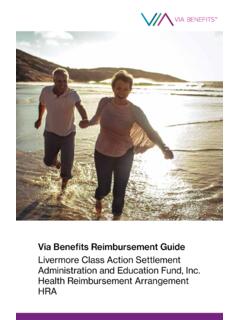
1 Recurring Premium Reimbursement form Mail: OneExchange, Box 25184, Lehigh Valley, PA 18002-5184 Fax: (866) 886-0879. Faster, More Convenient, and Green! Skip paper - visit to file electronically. Account Holder SSN (No dashes) Former Employer Name Total Pages Account Holder Last Name First Name Email Address Daytime Phone # (No Dashes). Action Name & Relationship Premium Type Start Date End Date Amount New John Doe - Spouse Medical 01/01/20XX 12/31/20XX $ By signing below, I certify that the information provided on this Reimbursement request form is correct and that the premiums for which I am requesting or for which I. am providing validation: were incurred for premiums for the covered participant while eligible under the plan on or after its effective date, have not been reimbursed in any other way from any other source, and will not be submitted for future Reimbursement .
2 Upon receiving notice of a change in Premium or a cancellation of coverage, I will notify One Exchange within a suitable time period. Account Holder Signature Date To qualify for your Reimbursement Does your documentation cover these items? you must provide a third party Covered Participant's Name document that includes the ( John Doe). information to the right. Please Premium Type ( Medical). Date of Service CHECK Each Reimbursement ( 01/01/20XX thru 12/31/20XX). request Qualification as you complete Monthly Amount ( $ ). them. Name of Provider ( AARP). 300006-160815-FRMPSH- Recurring Premium Reimbur form AC. Guide to Requesting Recurring Premium Reimbursement Recurring Premium Reimbursement is an Monthly Amount: This amount must match option available to those who do NOT have the amount on the supporting document.
3 Automatic Reimbursement available on a Certification Requirement: Carefully read policy. the certification requirements before Submit one specialized Reimbursement signing. form at the beginning of the year to setup Documenting Your Premium Recurring Reimbursement for the following Reimbursement request : All Premium twelve months. There will be no need to file Reimbursement requests require third party a Reimbursement request again until the documentation showing each item below: following year. Covered Participant's Name Premiums must be a fixed monthly amount ( John Doe). for a set period of time. Recurring Premium Premium Type ( Medical). requests must be resubmitted each Date of Service calendar year. ( 01/01/20XX thru 12/31/20XX). Account Holder Information: The Monthly Amount ( $ ).
4 Account holder is usually the retiree or Name of Provider ( AARP). spouse. For Medicare premiums deducted from your Reimbursement request Information: Social Security check, use the Social This section must be completed with a line Security Benefit Award Letter issued by the for each Premium Reimbursement Social Security Administration (SSA) each requested. year, usually during the month of October Action: A request must be submitted each or November, as your third party time you have a new policy, at the first of a documentation. Watch for this document to new year, when a change in your Premium arrive in the mail. occurs or if a policy ends for any reason during the calendar year. Enter: New For lost documents you can request a Policy , Premium Change or End of Proof of Income letter by contacting the Policy.
5 Social Security Administration at Relationship: Include the relationship 1-800-772-1213 (TTY 1-800-325-0778) or between the account holder and the person , or contact your insurance requesting the Premium Reimbursement carrier and request a document that ( self). contains the five items listed above. Premium Type: Refer to your Eligible Expense Insert ( Medical). Direct Deposit! Why wait for a check? Start Date: This is usually January 1st of Expedite your payments by signing up for each new year or the effective date of the direct deposit today. Refer to your Welcome coverage period, such as when a participant Kit for instructions on how to log into the becomes Medicare-eligible. portal. End Date: This is usually December 31st, or could be earlier if there is a death of a covered participant.
6 300006-160815-FRMPSH- Recurring Premium Reimbur form AC.