Transcription of STANDARDIZED PROVIDER INFORMATION CHANGE FORM
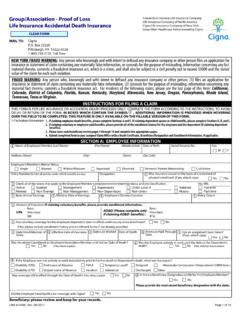
1 STANDARDIZEDPROVIDERINFORMATIONCHANGEFOR MCOMPLETE ALL APPLICABLE INFORMATION AND UTILIZE SUBMIT BUTTON FOR NEW PROVIDERS,CONTRACTUALMODIFICATIONS,OR CREDENTIALING CHANGES1of 2*2. PROVIDER INFORMATION :*Section requiredLast Name:First Name:MiddleInitial: PROVIDER Former Name(if applicable):Gender: Male FemalePrimary Specialty:INDNPI:INDTAX ID:EPSDT (If applicable) : Yes NoAccept Medicare & Medicaid: Yes NoHospital Accreditation:Hospital Affiliation 1:2:3:Board Certification 1:2:3:Language 1:2:3: PROVIDER Type: PCP Ancillary BehaviorHealth Facility LTSS SpecialistAddress Line 1:Address Line 2:City:State:County:Zip Code: PROVIDER Email Address:3. ADDRESS INFORMATION (If adding or changingTIN or Group NPI, please include a copy of the W9.)Product: MA MMP Medicaid All ProductsGroup Name:Group NPI:GroupTAX ID:ENTER NEW OR ADDITIONAL ADDRESS BELOWENTER OLD ADDRESSES TO BE TERMINATED BELOWA ddress Type: PrimaryService SecondaryService CorrespondenceAddress Type: PrimaryService SecondaryService CorrespondenceAddress Line 1:Address Line 1:Address Line 2:Address Line 2:City:City:State:County:Zip:State:Count y:Zip:Phone: Fax:Phone: Fax: INFORMATION RELATED TO NEW OR ADDITIONAL SERVICE LOCATIONH ours of Operation:MondayTuesdayWednesdayThursday FridaySaturdaySundayOpen:Close.
2 Patient Center Medical Home Yes NoLocation marked and visible from street Yes NoLocation easily accessible via public transportation Yes NoAccessible to members with disabilities Yes NoDesignated parking for disabled Yes NoRestrooms accessible for people with disabilities Yes NoWheelchair ramps Yes NoAuto-open external doors Yes NoWaiting room accommodate patients in wheelchairs/scooters Yes NoExam rooms with accessible equipment Yes NoIf radiology offered, accessible to disabled patients Yes NoADA compliance on service animals Yes NoMaterials available in braille and large print Yes NoASL interpretation available Yes No*1. INDICATE CHANGE (S) BEING SUBMITTED: Checkallthat apply(*Sections 1,2 and 5 arerequired.)Please include effective date for each item checked. PROVIDER INFORMATION (Complete sections 2,3,5)Effective Date:_____ Panel Status(Complete sections 2,4,5)EffectiveDate:_____ Address INFORMATION (Complete sections 2,3,5)EffectiveDate:_____ Group Name(Complete sections 2,5)EffectiveDate:_____Indicate documents included: PROVIDER Roster Other(List):IF APPLICABLE, PLEASE ATTACH A SEPARATE LIST WITH THE NAMES AND NPI NUMBERSOF ALL OF THE PROVIDERS IN THIS GROUP FOR WHOM THE ADDRESS CHANGE IS ALL APPLICABLE INFORMATION AND UTILIZE SUBMIT BUTTON FOR NEW PROVIDERS,CONTRACTUALMODIFICATIONS,OR CREDENTIALING CHANGES2of 2 All Cigna products and services are provided exclusively by or through operating subsidiaries of Cigna Cignaname, logos, and other Cigna marks are owned by Cigna Intellectual Property, Inc.
3 2016 INT_16_41716032420163. ADDRESS INFORMATION (If adding or changing TIN or Group NPI, please include a copy of the W9.)Product: MA MMP Medicaid All ProductsGroup Name:Group NPI:GroupTAX ID:ENTER NEW OR ADDITIONAL ADDRESS BELOWENTER OLDADDRESSES TO BE TERMINATED BELOWA ddress Type: PrimaryService SecondaryService CorrespondenceAddress Type: PrimaryService SecondaryService CorrespondenceAddress Line 1:Address Line 1:AddressLine 2:Address Line 2:City:City:State:County:Zip:State:Count y:Zip:Phone:Fax:Phone: Fax: INFORMATION RELATED TO NEW OR ADDITIONAL SERVICE LOCATIONH ours of Operation:MondayTuesdayWednesdayThursday FridaySaturdaySundayOpen:Close:Patient Center Medical Home Yes NoLocation marked and visible from street Yes NoLocation easily accessible via public transportation Yes NoAccessible to members with disabilities Yes NoDesignated parking for disabled Yes NoRestrooms accessible for people with disabilities Yes NoWheelchair ramps Yes NoAuto-open external doors Yes NoWaiting room accommodate patients in wheelchairs/scooters Yes NoExam rooms with accessible equipment Yes NoIf radiology offered, accessible to disabled patients Yes NoADA compliance on service animals Yes NoMaterials available in braille and large print Yes NoASL interpretation available Yes No4.
4 PRIMARY CARE PANEL STATUS:May be impacted by contract terms and follow-upmay be required. Openpanel Closepanel Nursing homeonly Accepting existing patientsonlyOther(pleasespecify):_____*5 . CONTACT PERSON SUBMITTING INFORMATION :*Section :Title:Phone:Fax:Email:Dateof Submission.