Transcription of Subchondral Bone Cysts - The Podiatry Institute
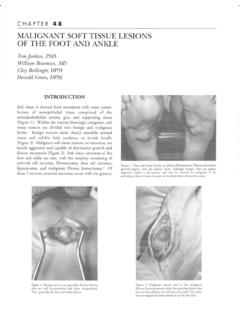
1 CHAPTER 44 SUBCI_IONDRAL BONE CYSTSS tepben J. Miller, , Cysts found in the sub-articular bone adjacent tojoints afflicted by osteoarthritis or rheumatoidarthritis were identified and described by Plewes in1940, Coliins in 7949, and Landells in 1953 (Fig. 1).Figure 1. Sub-articular bone cyst in the metatarsal head of patient withrheumatoid , related Subchondral bone Cysts with asynovial-like lining were subsequently described byFisk in 7949 and Hicks h 7955. Over the years, var-ious synonyms for these lesions have appeared inthe literature: synovial Cysts , juxta-articular bonecysts, intra-osseous ganglia, ganglion Cysts of bone,and to the \X/orld Health Organizationclassification of bone tumors and tumor-likelesions, the term juxta-afiicular bone cyst (intra-osseous ganglion) is defined as "a benign cysticand often multi-loculated lesion made up of fibroustissue, with extensive mucoid changes, located inthe Subchondral bone adjacent to a , it appears as a well-defined oste-olyic lesion with a surrounding area of sclerosis.
2 Ithas been described as a synovial cyst , but it lacks asynovial lining." As such, the definition excludesthe cystic juxta-articular bone lesions seen in con-junction with pigmented villonodular synovitis, aswell as other osteolyic bone spite of the great number of descriptivenames, these lesions share virtually the samemacroscopic and microscopic characteristics. Thecysts are usually solitary, but may be commonly develop in the epiphyseal or meta-physeal areas of bone adjacent to joints. Generally,they have a whitish or bluish lining consisting ofparallel bundles of collagen. The fibrocyes lyingalong the inner wall of the cavity sometimes forman incomplete lining of flattened, synovial-likecells. This makes for a smooth wall within whichthe cyst contains a thick gelatinous mucoid , there are those who distinguish thesubchondral bone Cysts seen in conjunction withosteoarthritis or other joint damage, from intra-osseous ganglia or synovial Cysts of bone.
3 Theformer are more likely to communicate with thejoint through the articular surface in up to 400/o ofthe cases, and therefore may be filled with synovialfluid; whereas the latter communicate with the jointin less than 3o/o of the documented cases and thefluid is more commonly a viscous mucoid fact, the Armed Forces Institute of Pathology, aslate as 1977, separated as distinct entities the sub-chondral bone Cysts and the synovial cyst of similar cystic lesions are found in con-junction with silastic joint implants (Fig. 2), and asa consequence of the degenerative changes causedby osteochondral fractures such as those seen inthe ankle 2. Silastic implant clegeneration resulting in periarticularmultilocular r:vst 44 PATHOGENESISMany theories have been proposed to describe thegenesis of these lesions.
4 The early theories of "syn-ovial fluid intrusion," either as a primary event fromincreased intra-articular pressure, or as a secondaryevent during the healing process when necroticsubchondral bone is removed, is more applicableto the Subchondral bone cyst associated witharthritic contrast, it is believed that the intra-osseousganglion is caused by a primary intramedullarymetaplasia of the mesenchymal cells into synovial-like cells and/or fibroblasts. This transformation isaccompanied by clegenerative changes creating themucin-like substance which is rich in hyaluronicacid. The role of trauma and compressive forces hasbeen postulated, but the association remains bone Cysts associated with arthritis(especially rheumatoid arthritis) occur in the sub-afiicular bone adjacent to joints. In the lowerextremity, they are most commonly found in themetatarsal heads.
5 Intra-osseous ganglia occur nearjoinls, and in the lower exlremity they more com-monly occur in the medial malleolus, proximal fibula,proximal tibia, as well as the tarsus area and bone Cysts are well known tooccur in the first metatarsal head, particulady near themedial eminence in association with hallux is commonly true even when there are no radi-ographically identifiable changes in the joint (Fig. 3).Figurc 3. Subchondral bone Cysts associated with halluxabductovalgus the recent literature, a sunrey by Murff andAshry of intraosseous ganglia identified of 273lesions: 430/o were found in women and 57o/o inmen, with an averaple age of 4J years. The mostcommon site was in the lower extremity, especiallythe distal tibia (Table 1).Table 1 LOCATIONS OFINTRAOSSEOUS GANGLIAU pper Extremity 68 Lower Extremity 745 Above Knee 41 Below Knee 101 Prox.
6 Tibia 30 Mid Tibia 1 Medial Malleolus 39 Prox. Fibula 8 Lateral Malleolus 5 Talus 7 Tarsus 71st Metatarsal 2 Great Toe 1(n: 213)Murff and Ashry JFAS, 199,iAlthough cystic bone lesions may be asymp-tomatic, they commonly cause intermittent painaggravated by increased activity. Joint movementby itself does not necessarily calise pain. The dis-comfort is thought to be caused by an increasedintra-lesional pressure from the accumulation offluid. However, on rare occasions, pain may resultfrom fracture through the Subchondral bone. Theselesions tend to weaken the surrounding bone. Ifthere is communication between the cyst and thejoint, then the synovial fluid may move back andforth between the , pain precedes the radiographicappearance of the lesion. Moreover, sr,rbchondralbone Cysts have been repofied to occur precedingthe subsequent diagnosis of inflammatory ordegenerative the radiograph, the lesion usually appearsas a well-demarcated circular to oval radiolucentdefect outlined by a thin margin of sclerotic bone,usually rreaf a joint.
7 It may be multilocular, but ismore commonly unilocular with varying dimen-sions, ranging from a few millimeters up to severalCHAPTER 44233centimeters in diameter. There is no cortical expan-sion or periosteal proliferation that occurs due tothe presence of these tomography (CT) can better delin-eate the extent of the lesion within the bone, andmay help determine if it communicates with theioint (Fig. 4). However, to better determine the softtissue components, as well as the nature of thefluid within the cyst , magnetic resonance imaging(MRI) is a more precise diagnostic test. The T2-weighted images, in particular, clearly depict thesynovial fluid demonstrated lry a high signalintensity, and differentiate it from the cartilagewhich is of lower signal intensity. On T1-weightedimages, the cyst is usually of low to intermediatesignal intensity, and is surrounded by a very 1owsignal intensity rim.
8 On T2-weighted and short T1inversion recovery images, the cyst is well-definedand is of a very high signal intensity, due to thepresence of ,u-e 4. CT scan iilustratin i bone Cysts in thc flrst mctatarsal heacland adjacent sesamoid bones, cornmunicating with the DiagnosisSince these intra-osseous Cysts are similar to otherlesions of bone, a differential diagnosis must bedeveloped (Table 2). The aneurysmal bone cyst ,giant cell tllmor, ancl chondromloroid fibroma usu-ally cause some expansion of the cortex or aperiosteal reaction. Cartilage tumors generallydemonstrate intralesional calcification; a findingthat is rarely present in intra-osseous 2 DIFFERENTIAT DIAGNOSISSI.]BCHONDRAL BONE CYSTSA rthritic CystsUnicameral Bone CystsOther Epiphyseal, Osteolyic Bone Lesions:ChondroblastomaChrondromaDermoid FibrorrraOsteoid OsteomaBrodie's AbscessTuberculosisPigmented Villonodular SynovitisUnicameral bone Cysts are predominantlyfound in the central shafts of long bones or bodiesof short bones (Fig.)
9 5) other considerationsinclude Rrodie's abscess associated withFigure 5. L1nicameral bone cyst in calcaneus. Unlike most intraosseousg:rnglia, it is not near a , ancl pigmented villonodular synovi-tis, which generally shows erosive lesions on eachside of the joint. Occasionally, a systemic diseasesuch as tuberculosis can procluce osteolotic lesionsof bone that resemble Subchondral bone rysts (Fig. 6).234 CHAPTER 44 Figure 6. Cystic lesion caused by bone Cysts associated with arthritis orafihrosis can improve with intra-afiicular steroidinjection. The increased pressure can be relievedby aspirations of the cyst , with or wlthout the sub-sequent injection of corticosteroid the true intra-osseous ganglia, the lesion can beaspirated and injected quite similar to soft tissueganglia. However, the incidence of recurrence ofsymptoms is relatively high.
10 \X/hen symptoms persist in spite of conserwa-tive treatment, the usual surgical approach consistsof excision of the bone cyst . Curettage is utilizedto remove any remaining components of the softtissue lesion along with the surrounding zone ofsclerosis. This is followed by packing of the defectwith suitable bone grafting material, usually in theform of allogenic cancellous bone chips. If thismaterial is not available, then a bone substitutemay be cortical bone covering the subchondralbone cyst should be removed as a plate, so that itcan be replaced after the lesion is excised andpacked with bone. The success rate of curettageand packing is very high, with only a 7o/o recur-rence rate reported for intra-osseous various joint procedures are being con-sidered, in the presence of Subchondral bone cystsor intra-osseous ganglia, some special considera-tions are warranted.