Transcription of TECHNIQUESOFTHEEVANS CALCANEALOSTEOTOMY
1 INTRODUCTIONF irst used in 1961 to treat calcaneovalgus in a patient withpoliomyelitis, Dillwyn Evans applied his understanding ofthe medial and lateral columns and performed what is nowreferred to as the Evans calcaneal osteotomy (1). Nowroutinely used to correct both pediatric and adult pesplanovalgus deformities, the Evans procedure has beenproven a consistent method of treatment (2-14). Asdescribed by Evans, lengthening the lateral column allowspreservation of the calcaneo-cuboid joint while pushing thenavicular bone medially and so straightening the foot (1).First line therapy for pediatric pes planovalgus typicallyconsists of conservative measures to decrease pain andinstability. Orthotics, bracing, and nonsteroidal anti-inflammatory drugs may relieve symptoms short term,however severe deformities may best respond to surgicalintervention.
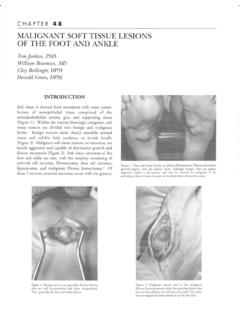
2 Historically, a variety of surgical procedures forpes planovalgus have been utilized, with most attentionplaced on the Evans calcaneal osteotomy. Since theprocedure was first introduced, a variety of surgicalvariations have been described and debated. Differentincisional approaches, distraction devices, fixation choices,and bone graft options have been tested, though muchof the procedure s technique can be traced back to Evanshimself (2-14). From the senior author s years of experience,the following technique has been refined and provenhighly TECHNIQUEThe Evans calcaneal osteotomy is usually performed undergeneral anesthesia with a mid-calf tourniquet, unless doing oblique incision (Figure 1) approximately 4 cm inlength is made over the lateral aspect of the placement is crucial for adequate exposure of theosteotomy and graft insertion.
3 Incisional landmarks includethe anterior beak of the calcaneus distally, and the inferiorsurface of the calcaneus proximally. The location of theplanned osteotomy, approximately 1 cm proximal to thecalcaneal-cuboid joint, should be the center of the is deepened through the subcutaneoustissue, taking care to either cauterize or tie off any of thesuperficial crossing working with children, it is important toremember the delicate nature of their tissues. Especially inthis anatomic area, the subcutaneous layer is particularly thin(Figure 2). The subcutaneous tissue is elevated from thesurface of the deep fascia in a circumferential manner toTECHNIQUES OF THE EVANSCALCANEAL OSTEOTOMYA llison Menke, DPMJohn Ruch, DPMCHAPTER5 Figure 1. Incision 2. Subcutaneous tissue the majority of the extensor digitorum muscle belly(EDB).
4 This dissection is not extended inferiorly over theperoneal tendons. The subcutaneous layer overlying thetendons is undermined without dividing the tissue and aRagnell retractor is inserted inferiorly to protect the suralnerve (Figure 3). Adequate reflection of the superficialfascia gives linear access to the lateral aspect of the calcaneuslying beneath the EDB deep fascia is then incised along the inferior marginof the EDB muscle, above the course of the peronealtendons. The Ragnell retractor is then reinserted beneaththe peroneal tendons to expose the periosteal surface of theinferior lateral calcaneal wall. The EDB muscle belly is thengently separated and retracted from the dorsolateral aspect ofthe calcaneal cuboid joint and wall of the calcaneus (Figure4). Proximal attachments of the EDB may need to bereleased over the entrance to the sinus reflection of the extensor digitorum muscle bellysuperiorly and the peroneal tendons inferiorly, the lateralaspect of the calcaneus is exposed (Figure 5).
5 Next, thecalcaneal-cuboid joint is identified. A Freer elevator is in-troduced into the joint (Figure 6) to appreciate itsorientation and alignment. The osteotomy must be madeparallel to the calcaneal-cuboid the obliquity of the joint is visualized, a periostealincision is made approximately one centimeter proximal andparallel to the calcaneal-cuboid joint (Figure 7). A Freerelevator is used to reflect the periosteum several millimetersin the proximal direction from the incision line. Theperiosteum is specifically left intact distally as to avoiddisruption of the dorsal calcaneal-cuboid joint this point, a sagittal saw is used to cut the CALCANEALOSTEOTOMY . The osteotomy is made approximately 1 cmproximal, and parallel, to the calcaneal-cuboid joint(Figure 8). The osteotomy technique includes cutting ofthe lateral, dorsal and plantar cortices.
6 The medial cortexof the calcaneus is contacted but not transected, creatinga stable hinge for distracting of the AO mini-distractor is inserted to distract theosteotomy. Then inch Kirschner wires are inserted oneither side of the osteotomy in a dorsolateral to plantar-medial orientation. The osteotomy is then dialed openCHAPTER 520 Figure 3. Protection of peroneal tendons and sural 4. Reflection of EDB muscle 5. Exposed lateral calcaneal 6. Identification of the calcaneo-cuboid one centimeter and range of motion of thesubtalar and midtarsal joints is evaluated. With adequatecorrection, the talar head should be captured securely withinthe medial rim of the navicular. This can be assessed withboth manual manipulation and intraoperative the desired amount of correction is attained, thewidth and depth of the distracted osteotomy are measured(Figure 9).
7 A piece of iliac crest allograft is then fashioned tofit the open defect of the calcaneus. A truncated wedgetypically provides the best fit, as it mirrors the internal shapeof thecalcaneus (Figures 10, 11).Onceprepared,the graftisinsertedintothedistractedosteotom yandgentlytappedintoplace with a mallet and tamp. The graft should be implantedso that it is not proud, rather resting within the walls of thesurrounding calcanues (Figures 12, 13). The distractor isthen dialed closed and removed. If the osteotomy and graftare stable, no internal fixation device has been found to benecessary. The final outcome is then reassessed by clinicalmanipulation and intraoperative 3-0 absorbable suture is used to close the EDBmuscle belly over the lateral calcaneus and bone graft(Figure 14). The rich vascularity and migration ofmesenchymal cells from the muscle tissue provide an optimalenvironment for graft incorporation within the calcaneus(15).
8 The subcutaneous layer is then re-approximated withan absorbable 4-0 suture and the skin re-approximated withan absorbable 5-0 subcuticular , a sterile dressing and below-kneeJones compression cast are applied. Within one week,the initial dressing is removed and a permanent castapplied if swelling has resolved and the wound status isacceptable. Patients should be kept non-weightbearing forapproximately 6 weeks, after which they can be transitionedto a walking correcting pes valgus deformities, a variety ofadjunctive procedures are often necessary and coupled withthe Evans osteotomy. Most commonly utilized proceduresinclude gastrocnemius recession, Young s tendonsuspension, cotton osteotomy, and medial column 521 Figure 7. Periosteal 8. Osteotomy, 1cm proximal and parallel to the 9. Measuring for the appropriate-sized 10.
9 Fashioning the Evans D. Calcaneo-valgus deformity. J Bone Joint Surg1975;57 Mahan KT, McGlamry ED. Evans calcaneal osteotomy for flexiblepes valgus deformity. Clin Podiatr Med Surg 1987;4:137 513. Roye DP, Raimondo RA. Surgical treatment of the child s andadolescent s flexible flatfoot. Clin Podiatr Med Surg 2000;17 Dolan CM, Henning JA, Anderson JG, Bohay DR, Kornmesser MJ,Endres TJ. Randomized prospective study comparing tri-cortical iliaccrest auto graft to allograft in the lateral column lengtheningcomponenet for operative correction of adult acquired flatfootdeformity. Foot Ankle Int 2007;28 Dogan A, Zorer G, Mumcuoglu EL, Akman EY. A comparison oftwo different techniques in the surgical treatment of flexible pesplanovalgus: calcaneal lengthening and extra-articular subtalararthrodesis. J Pediatr Orthop B 2009;18 Mosier-LaClair S, Pomeroy G, Manoli A.
10 Operative treatment of thedifficult stage 2 adult acquired flatfoot deformity. Foot Ankle Int2001;6 Zwipp H, Rammelt S. Modified Evans osteotomy for the operativetreatment of acquired pes planovalgus. Oper Orthop Traumatol2006;2 Gallina J, Sands AK. Lateral-sided bony procedures. Foot Ankle Int2003;3 Soomekh DJ, Baravarian B. Pediatric and adult flatfoot reconstruction:subtalar arthroereisis versus realignment osteotomy surgical Podiatr Med Surg 2006;4 Hix J, Kim C, Mendicino RW Saltrick K, Catanzariti AR. Calcanealosteotomies for the treatment of adult-acquired flatfoot. ClinPodiatr Med Surg 2007;24 Weinraub GM, Daulat R. The Evans osteotomy: technique andfixation with cortical bone pin. J Foot Ankle Surg 2001;40 Viegas GV. Reconstruction of the pediatric flexible planovalgusfoot by using an Evans calcaneal osteotomy and augmentative medialsplit tibialis anterior tendon transfer.